The birth of a healthy child is the natural desire of every pregnant woman. But, unfortunately, hopes for happy motherhood are not always justified. About 5% of newborns have various congenital diseases. Screening in the 1st and 2nd trimesters of pregnancy allows you to determine how high the risk of congenital pathology is in the unborn child.
Currently, there are quite effective methods for prenatal (prenatal) diagnosis of many fetal diseases that can be detected from the 11th week of pregnancy. Timely screening examinations make it possible to identify a wide range of fetal pathologies and see ultrasound signs of chromosomal abnormalities.
What is early prenatal screening and when is it performed?
Screening (from the English “sifting”) is a set of studies that allows us to identify groups of pregnant women who are at risk of having a child with chromosomal abnormalities and congenital defects. But early screening is only the initial, preliminary stage of the examination, after which women with an identified risk of congenital anomalies are recommended to have a more detailed diagnostic examination that will accurately confirm or exclude the presence of pathology.
This diagnostic complex is carried out for pregnant women at a period of 11–13 weeks + 6 days (when the coccygeal-parietal size of the fetus is from 45 to 84 mm). The most optimal time for screening is considered to be from 12 to 13 weeks, since such an examination evaluates both the signs of chromosomal pathology in the fetus and the anatomical structures of the unborn child, and at a period of 11 weeks - 11 weeks + 4 days it is very difficult to do this .
What does early prenatal screening include?
A comprehensive examination includes:
- Ultrasound of the fetus for the presence of markers (signs) of chromosomal pathology and congenital malformations;
- determination of the level of biochemical markers of chromosomal abnormalities in the blood of a pregnant woman: beta-hCG and PAPP-A. The study is carried out on special high-tech equipment Cobas e, Roshe, approved for calculating the risk of chromosomal syndromes in the Astraia (FMF) program;
- Doppler ultrasound of the uterine arteries
- cervicometry – measurement of the length of the cervix;
- collecting anamnesis (age, height, weight, number of pregnancies and births, smoking, diabetes, arterial hypertension, etc.);
- measuring blood pressure in both arms.
The data obtained: medical history, ultrasound and biochemical markers are placed in a specially developed Astraia program, which calculates the risk of having a child with congenital anomalies. The combination of these studies increases the efficiency of identifying fetuses with Down syndrome and other chromosomal diseases.
What is the Astraia program
Astraia is a professional program that calculates the likelihood of chromosomal abnormalities in a fetus. The program was developed by the Fetal Medicine Foundation (FMF) in London and was successfully tested on a huge amount of clinical material in many countries around the world. It is constantly being improved under the leadership of a leading specialist in the field of prenatal diagnostics, Professor Kypros Nicolaides, in accordance with the latest world advances in the field of fetal medicine.
The specialist conducting early prenatal screening must have an international FMF certificate, which gives the right to perform this diagnosis and work with the Astraia program. The certificate is confirmed annually after a statistical audit of the work done during the year and passing the certification exam. This ensures high diagnostic accuracy of the obtained risks.
Conducting early prenatal screening using this program is regulated by Order of the Ministry of Health of the Russian Federation dated November 1, 2012 No. 572n “On approval of the procedure for providing medical care in the field of obstetrics and gynecology (except for the use of assisted reproductive technologies).”
Early prenatal screening allows you to calculate the following risks:
- Down syndrome (trisomy 21) in the fetus;
- Edward syndrome (trisomy 18) in the fetus;
- Patau syndrome (trisomy 13) in the fetus;
- the risk of developing early (before 34 weeks) and late (after 37 weeks) preeclampsia (preeclampsia) in the pregnant woman herself.
What is assessed during ultrasound in the 1st trimester
Coccygeal-parietal size (CPS) of the fetus
This indicator accurately determines the gestational age (pregnancy), especially if a woman does not remember the 1st day of her last menstruation, or if her menstrual cycle is not regular. In conclusion, the gestational age is set according to the fetal calf temperature, and not according to the date of the last menstruation.
Correct measurement of fetal CTE
Markers of chromosomal pathology:
- nuchal translucency thickness (TN) is the main sign of chromosomal pathology in the fetus. A pathological value is considered to be an increase in TVP greater than the 95th percentile for each gestational age. Each increase in TVP increases the risk of a chromosomal abnormality in the fetus.
TVP is normal TVP is pathological
It is important to understand that an increase in TVP is a sign (marker), but not an accurate diagnosis of chromosomal abnormalities in the fetus. Only invasive diagnostics followed by genetic analysis can determine the presence of Down syndrome and other diseases in an unborn child.
- nasal bone. In fetuses with Down syndrome, the nasal bone may be absent or reduced in size (hypoplastic). Very rarely, this can occur in completely healthy children. An accurate diagnosis can only be established using genetic analysis.
Normal nasal bone Absent nasal bone
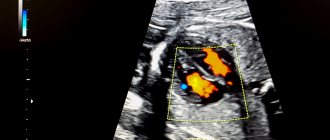
- blood flow in the ductus venosus is a small vessel in the fetal liver. With reverse (retrograde) blood flow in this vessel, it can be assumed that the fetus has a chromosomal syndrome or a congenital heart defect.
Normal blood flow in the ductus venosus
But it is important to correctly obtain this blood flow and evaluate it. This requires certain skills and qualifications of a doctor, which are confirmed by annual FMF certification.
- blood flow through the tricuspid valve into the fetal heart. Here, retrograde (reverse) blood flow also indicates a chromosomal pathology, or can manifest itself in congenital heart defects.
Anatomical structures of the fetus and exclusion of major congenital defects
Fetal hand Fetal brain in the form of a “butterfly” is normal
Cervical length
Walls of the uterus and appendages (ovaries)
Blood flow in the uterine arteries
Ultrasound can be performed either transabdominally or transvaginally.
If an ultrasound examination reveals markers of fetal chromosomal pathology
- Dear patients, first of all, we ask you to remember the most important thing: if markers (signs) of chromosomal pathology of the fetus were found during an ultrasound examination, this does not mean that the fetus has a chromosomal pathology, and the pregnancy must be terminated.
- All women who have been found to have ultrasound markers of chromosomal pathology of the fetus are offered invasive prenatal diagnostics - today, depending on the stage of pregnancy, we offer three types of invasive diagnostics: chorionic villus aspiration (performed at 11-14 weeks), amniocentesis (16-18 weeks), cordocentesis (19-20 weeks). More information about invasive diagnostic methods can be found at this link.
The most common ultrasound markers of chromosomal abnormalities are:
Increase in TVP.
This parameter is assessed at the first screening ultrasound (11-14 weeks)
TVP (thickness of the collar space) may be greater than normal for several reasons.
Why may the fetus exhibit an increase in TVP?
Parents are extremely excited and want to immediately get answers to all the questions they have - what is involved, what to do, and many others. Questions that cannot be answered immediately. After all, there are many reasons for the increase in TVP. This finding can occur in completely healthy fetuses; this is not a developmental defect, it is only a signal for a more in-depth examination, because such a feature can occur in fetuses with chromosomal abnormalities, heart abnormalities, or other congenital or hereditary diseases. When increasing the maximum TVP threshold, it is IMPORTANT that the doctor evaluates all other ultrasound markers (signs) and also conducts a detailed assessment of the fetal anatomy. Perhaps the reason for the increase in TVP lies in a violation of fetal development (for example, abnormalities in the structure of the heart).
What to do if an increase in TVP is detected in the fetus?
If your fetus is diagnosed with an enlarged TVP, you will definitely be referred for a consultation with a geneticist, who, after collecting an anamnesis, assessing all the risks, will give recommendations on additional research methods (invasive diagnostics). Next, an expert ultrasound of the fetus will be required at 20 weeks for a detailed assessment of the anatomy. If all these studies do not reveal any deviations, then the chances of giving birth to a healthy child are high even with a significant amount of TVP.
Hypoplasia/aplasia of the nasal bones.
Hypoplasia of the nasal bones is a reduction in the size of the nasal bone depending on the CTE of your baby.
Aplasia of the nasal bones is the lack of visualization of your baby's nasal bone.
The lack of visibility of the bony part of the nasal dorsum in the fetus or its underdevelopment (not bright enough) at the first screening is associated with delayed calcium deposition. This situation may be somewhat more common in fetuses with Down syndrome, but it is important that:
- the absence of nasal bones on ultrasound is not a developmental anomaly in itself; can occur in completely healthy fetuses (in 3% of cases);
- to assess the degree of individual risk, it is necessary to evaluate the remaining ultrasound markers (thickness of the fetal nuchal translucency, blood flow indicators on the heart valve, blood flow indicators in the ductus venosus, fetal heart rate) and biochemical analysis of maternal serum (PAPP-A, hCG);
- If the result of a combined screening (evaluation of ultrasound and blood test data in a special program) shows a LOW risk of chromosomal pathology, there is no need to worry. Be sure to undergo a follow-up ultrasound at 19-20 weeks of pregnancy, where a thorough assessment of the fetal anatomy will be carried out and certain ultrasound markers of the second trimester of pregnancy will be examined.
- What to do if the combined screening result is HIGH? – There’s no need to worry. You will definitely be referred for a consultation with a geneticist, who, having collected an anamnesis, assessed all the risks, will give recommendations on additional research methods (invasive diagnostics).
Hyperechoic intestine.
This is a term that refers to increased echogenicity (brightness) of the intestine on an ultrasound image. The finding of hyperechoic bowel NOT a malformation of the bowel, but simply reflects the nature of its ultrasound image. It must be remembered that the echogenicity of the normal intestine is higher than the echogenicity of its neighboring organs (liver, kidneys, lungs), but such intestine is not considered hyperechoic. Only intestines whose echogenicity is comparable to the echogenicity of fetal bones are called hyperechoic.
Why can the fetal intestine be hyperechoic?
Sometimes hyperechoic intestine is detected in completely normal fetuses, and this sign may disappear with dynamic ultrasound. Increased echogenicity of the intestine may be a manifestation of chromosomal diseases of the fetus, in particular Down syndrome. Therefore, when hyperechoic bowel is detected, a careful assessment of fetal anatomy is performed. However, if a hyperechoic intestine is detected, we can only talk about an increased risk of Down syndrome, since such changes can also occur in completely healthy fetuses. Sometimes hyperechoic bowel may be a sign of intrauterine fetal infection. Hyperechoic bowel is often found in fetuses with intrauterine growth restriction. However, this will necessarily reveal a lag in the size of the fetus from the gestational age, oligohydramnios, and impaired blood flow in the vessels of the fetus and uterus. If none of the above is detected, then the diagnosis of fetal growth restriction is excluded.
What to do if hyperechoic intestine is detected in the fetus?
You should contact a genetic specialist who will once again evaluate the results of biochemical screening and give the necessary recommendations for further management of pregnancy.
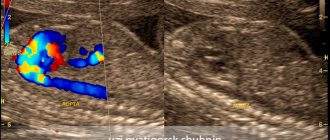
Hyperechoic focus in the ventricle of the heart.
This is a term that refers to the increased echogenicity (brightness) of a small area of the heart muscle on an ultrasound image. Identification of a hyperechoic focus in the heart NOT a cardiac malformation, but simply reflects the nature of its ultrasound image. A hyperechoic focus occurs at the site of increased deposition of calcium salts on one of the heart muscles, which does not interfere with the normal functioning of the fetal heart and does not require any treatment.
Why can a fetus have a hyperechoic focus in the heart?
Sometimes a hyperechoic focus in the heart is detected in completely normal fetuses, and this sign may disappear with dynamic ultrasound. The presence of a hyperechoic focus in the fetal heart may be a manifestation of fetal chromosomal diseases, in particular Down syndrome. In this regard, when a hyperechoic focus is detected, a careful assessment of the fetal anatomy is carried out. However, this marker refers to the “small” markers of Down syndrome, therefore, identifying only a hyperechoic focus in the heart does not increase the risk of having Down syndrome and is not an indication for other diagnostic procedures.
What to do if a hyperechoic focus is detected in the fetal heart?
If the fetus has ONLY a hyperechoic focus in the heart, then no additional examinations are required; the risk of Down's disease does not increase. At a planned ultrasound at 32-34 weeks, the fetal heart will be examined again. In most cases, the hyperechoic focus in the heart disappears by this stage of pregnancy, but even if it continues to remain in the heart, this does not in any way affect the health of the fetus and the management of pregnancy.
The only artery of the umbilical cord.
A normal umbilical cord consists of three vessels - two arteries and one vein. Sometimes, instead of two arteries, only one artery and one vein are formed in the umbilical cord, thus, only two vessels are identified in the umbilical cord. This condition is considered a malformation of the umbilical cord, but this defect does not have any effect on the postpartum condition of the child and its further development.
Why can a single umbilical cord artery be identified in a fetus?
Sometimes a single umbilical cord artery is identified in completely normal fetuses; After the birth of a child, this fact does not have any impact on its further development. Sometimes a single umbilical cord artery is combined with defects of the fetal cardiovascular system, therefore, when a single umbilical cord artery is identified, a detailed examination of the anatomy of the fetus and, in particular, the cardiovascular system is carried out. In the absence of other malformations, a single umbilical cord artery is able to provide adequate blood flow to the fetus. Somewhat more often, a single umbilical cord artery is detected in fetuses with Down syndrome and other chromosomal diseases. However, this marker is a “minor” marker of Down syndrome, so identifying only a single umbilical cord artery does not increase the risk of Down syndrome and is not an indication for other diagnostic procedures. A single umbilical cord artery sometimes leads to intrauterine growth retardation. In this regard, if a single umbilical cord artery is detected, an additional ultrasound is recommended at 26-28 weeks of pregnancy, and a planned one at 32-34 weeks. If a lag in the size of the fetus from the gestational age or disruption of blood flow in the vessels of the fetus and uterus is not detected, then the diagnosis of fetal growth retardation is excluded.
What to do if a single umbilical cord artery is identified in the fetus?
Identification of only a single umbilical cord artery does not increase the risk of Down syndrome and is not an indication for genetic counseling or other diagnostic procedures. A control ultrasound is required at 26-28 and 32 weeks of pregnancy to assess the rate of fetal growth and evaluate its functional state.
Choroid plexus cysts (CPC).
The choroid plexus is one of the first structures to appear in the fetal brain. It is a complex structure, and the presence of both choroid plexuses confirms that both halves develop in the brain. The choroid plexus produces fluid that nourishes the brain and spinal cord. Sometimes the fluid forms collections inside the choroid plexus, which appear as a “cyst” on ultrasound. Choroid plexus cysts can sometimes be found on ultrasound between 18 and 22 weeks of pregnancy. The presence of cysts does not affect the development and function of the brain. Most cysts disappear spontaneously by 24-28 weeks of pregnancy.
Are choroid plexus cysts common?
In 1-2% of all normal pregnancies, the fetuses have CSS, in 50% of cases bilateral choroid plexus cysts are found, in 90% of cases the cysts spontaneously disappear by the 26th week of pregnancy, the number, size, and shape of cysts can vary, cysts are also found in healthy children and adults. Somewhat more often, choroid plexus cysts are detected in fetuses with chromosomal diseases, in particular with Edwards syndrome (trisomy 18, extra chromosome 18). However, with this disease, the fetus will always have multiple malformations, so identifying only choroid plexus cysts does not increase the risk of having trisomy 18 and is not an indication for other diagnostic procedures. In Down syndrome, choroid plexus cysts are usually not detected. The risk of Edwards syndrome when CSS is detected does not depend on the size of the cysts and their unilateral or bilateral location. Most cysts resolve by 24-28 weeks, so a control ultrasound is performed at 28 weeks. However, if choroid plexus cysts do not disappear by 28-30 weeks, this does not affect the further development of the child.
Enlargement of the renal pelvis (pyelectasia).
The renal pelvis is the cavity where urine from the kidneys collects. From the pelvis, urine moves to the ureters, through which it enters the bladder.
Pyeelectasia is an enlargement of the renal pelvis. Pyeelectasis is 3-5 times more common in boys than in girls. Both unilateral and bilateral pyeloectasia occur. Mild forms of pyelectasis often go away on their own, while severe forms sometimes require surgical treatment.
The cause of dilation of the renal pelvis in the fetus.
If there is an obstacle in the way of the natural outflow of urine, urine will accumulate above this obstacle, which will lead to expansion of the renal pelvis. Pyeelectasis in the fetus is diagnosed by routine ultrasound examination at 18-22 weeks of pregnancy.
Is pyeelectasis dangerous?
Moderate expansion of the renal pelvis, as a rule, does not affect the health of the unborn child. In most cases, during pregnancy, spontaneous disappearance of moderate pyelectasis is observed. Severe pyelectasis (more than 10 mm) indicates a significant difficulty in the outflow of urine from the kidney. Difficulty in the outflow of urine from the kidney may increase, causing compression, atrophy of the kidney tissue and decreased kidney function.
In addition, a violation of the outflow of urine is often accompanied by the addition of pyelonephritis, an inflammation of the kidney that worsens its condition. Slightly more often, dilation of the renal pelvis is detected in fetuses with Down syndrome. However, this marker refers to the “minor” markers of Down syndrome, therefore, detecting only dilation of the renal pelvis does not increase the risk of having Down syndrome and is not an indication for other diagnostic procedures. The only thing you need to do before giving birth is to undergo a control ultrasound at 32 weeks and once again assess the size of the renal pelvis.
Is it necessary to examine the baby after birth?
In many children, moderate pyelectasis disappears spontaneously as a result of the maturation of the urinary system after the birth of the child. For moderate pyelectasis, it may be sufficient to conduct regular ultrasound examinations every three months after the birth of the child. If a urinary infection occurs, antibiotics may be necessary. As the degree of pyelectasis increases, a more detailed urological examination is necessary.
In cases of severe pyelectasis, if the dilation of the pelvis progresses and a decrease in kidney function occurs, surgical treatment is indicated. Surgery can remove the obstruction to the flow of urine. Some surgical interventions can be successfully performed using endoscopic methods - without open surgery, using miniature instruments inserted through the urethra. In any case, the issue of surgical treatment is decided after the birth of the child and its complete examination.
What to do if ultrasound markers of chromosomal pathology are detected in the fetus?
You should contact a genetic specialist who will once again evaluate the results of ultrasound and biochemical screening, calculate the risk individually for your case and give the necessary recommendations for further management of pregnancy.
What is screening in the second trimester of pregnancy?
According to order No. 572n dated November 1, 2012, the second screening consists of an ultrasound examination of the fetus at 18-21 weeks of pregnancy. At this age, blood is no longer tested for biochemical markers. The fetus has a mass of about 300-500 grams and a length of 20-25 cm, and ultrasound allows you to analyze in detail all the anatomical structures of the fetus and identify most developmental defects. At the same time, the amount of amniotic fluid, the location and structure of the placenta, the length of the cervix, etc. are assessed.
After an ultrasound scan at these stages of pregnancy, most questions of prenatal diagnosis are considered closed.
We hope that this information will help you better understand the importance and necessity of screening in the first and second trimesters of pregnancy. In our clinic you have a unique opportunity to undergo a high-quality examination and obtain the most objective data about the condition of your fetus.
Sign up for prenatal screening at the Family Doctor clinic by phone in Moscow, through the online registration form or at the reception.
No more sentence! Congenital heart defects in children: identify and treat
Perhaps there will always be diseases about the methods of treatment of which one could say something like “If only such diagnosis and treatment existed... years ago.”
This phrase is also true in relation to our topic today. With Candidate of Medical Sciences, pediatric cardiologist at Clinic Expert Smolensk Tatyana Mikhailovna Frolova, we are talking about congenital heart defects.
— Tatyana Mikhailovna, what is congenital heart disease? Is this a separate disease or a group of diseases?
This is a whole group of pathologies - congenital defects in the structure of the heart and large vessels, as well as anomalies in the location of the heart in the chest. These defects disrupt blood flow inside the heart and in large vessels and can lead to the development of heart failure, disability, and in some cases, the death of the child.
Today there are more than 35 types of congenital heart defects
Today there are more than 35 types of such defects.
— Do babies with congenital heart disease always look different from their healthy peers? Or can a heart defect in a child be asymptomatic?
The latter is true. Along with very severe defects, there are also those that are not accompanied by obvious clinical manifestations. Such children may be no different from their peers. It has become possible to identify these defects thanks to the improvement of methods for studying the cardiovascular system. They are often diagnosed accidentally.
— How is it usually discovered that a child has a heart defect?
Modern ultrasound machines make it possible to detect or suspect the presence of fetal heart defects even in the prenatal period.
After birth, a child also undergoes an ultrasound examination of the heart in the first year of life.
“An ultrasound is definitely not enough. The examination must be comprehensive." Quote from the material “Ultrasound of the heart: when is it prescribed and what will it show?”
It is possible that a defect may be accidentally discovered during examination for other reasons (medical examinations, obtaining certificates for sports activities, etc.).
And, finally, situations when a child develops some symptoms or changes are detected on the ECG, which becomes a reason to deepen the diagnostic search and conduct echocardiography.
“What are the types of heart murmurs? Where do they come from? And what to do if such noise is detected? Quote from the material “Heart murmurs in a child: looking for reasons”
— Should a cardiac examination of a baby be carried out only when indicated, or should all newborns undergo special diagnostics to exclude congenital heart defects and other cardiovascular pathologies?
According to the order of the Ministry of Health, ultrasound screening (echocardiography) is mandatory at the end of the neonatal period (the first month of extrauterine life), i.e. when the baby is one month old, during a routine medical examination. All children under one year of age must undergo such a study along with an ECG.
Of course, if a child has any manifestations of trouble, they do not wait for any special time, but consult a doctor immediately.
— How many children in Russia and the world are born with congenital heart defects?
According to statistics, congenital heart defects are considered a fairly common pathology. Their frequency in our country is 8 children per 1000, or 1 per 125 live births. The true incidence is higher if we take into account cases of early stillbirths and cases of spontaneous abortions.
In European countries this figure ranges from 3 to 8 per 1000 children. The highest frequency is in third world countries, in Asian countries.
- Why is a child’s heart so vulnerable? Are heredity and ecology to blame, or are there other reasons for the development of congenital heart defects in babies?
Approximately 90% of heart defects are multifactorial in nature. In other words, the combined influence of both hereditary and environmental factors plays a role in their occurrence.
8% of defects are caused by chromosome abnormalities and “breakdowns” of individual genes.
In our country, 8 children out of 1000 are born with congenital heart defects
2% is due solely to environmental factors that increase the risk of congenital heart defects. These may be physical, chemical factors, hazardous production, or unfavorable environmental conditions.
In addition, the formation of the defect can be facilitated by maternal diseases (in particular, endocrine; infectious pathologies during pregnancy), taking certain medications, smoking, and drinking alcohol by the mother.
— Modern diagnostics make it possible to identify congenital heart defects at the stage of intrauterine development?
Yes, but not in all cases.
— Before birth, can any heart defects in the fetus be detected with 100% accuracy, or is the development of perinatal diagnostics imperfect today?
As I said earlier, reliable diagnosis is not always possible. The success of detecting a defect is influenced by the position of the fetus, its mobility during the examination, the qualifications and experience of the doctor, the class of the apparatus for performing ultrasound, and the severity of circulatory disorders.
Some anatomical features of the heart, such as a patent ductus arteriosus, are normal in the prenatal period and become a defect only if they persist for a long time after birth. In these cases, dynamic monitoring of the child comes first.
Why are pregnant women prescribed MRI? Read here
— Tatyana Mikhailovna, if a fetus is diagnosed with a heart defect, is this an indication for termination of pregnancy or is the decision made individually in each case?
Today this is not a reason to terminate a pregnancy. In Russia, individual operations for intrauterine correction of heart defects have already begun. If there are no indications for surgical treatment during pregnancy, then after the birth of the child and consultation with a cardiac surgeon, the necessary operation is performed either immediately or later.
— Previously, the diagnosis of “congenital heart disease” almost always sounded like a death sentence. Has the situation changed now?
Over the past 10-15 years - dramatically. What has changed? The detection of defects in the prenatal period has improved significantly. Defects began to be diagnosed that do not require urgent surgical intervention and that can be eliminated on their own as the child grows older. If there is a question about surgery, then, if necessary, it can be performed even on the first day after the birth of the child.
“Holter monitoring is also used to examine children.” Quote from the material “Holter (24-hour) ECG monitoring - complete instructions for the patient”
— If a baby is diagnosed with a heart defect after birth, is this always an indication for surgery?
No. All heart defects require dynamic monitoring, since their spontaneous closure is possible, reducing the severity of circulatory disorders, as a result of which there is no need for surgical treatment. With some defects, the child can even engage in certain sports if there are no significant circulatory disorders.
— If necessary, can surgeries in Smolensk help a baby with a congenital heart defect, or are such children sent to large Russian cardiology centers?
Heart surgeries are high-tech and highly specialized medical care. They are performed only in large specialized clinics.
If necessary, the operation can be performed even on the first day after the birth of the child.
Smolensk patients can undergo surgery in Moscow or St. Petersburg, if we talk about regional proximity. In our city, unfortunately, such operations are not carried out.
— It is generally accepted that prevention can save you from many health problems. Is it possible to reduce the risk of having a child with a heart defect?
Yes. It is extremely important to remember the periods of heart development here. Its formation begins at the end of the 2nd week of pregnancy. By the 4th week, a two-chamber heart is formed, and by the 6th week the chambers separate to form a four-chambered heart.
Just thinking about these numbers is enough. Does every woman at two weeks (and even later) know about her pregnancy? No, whereas at this time the heart is laid and formed. If during this period there are unfavorable factors that we talked about earlier, the risk of developing a defect increases. Therefore, the most important prevention is planning and preparation for pregnancy. A woman must be healthy, she needs to lead an appropriate lifestyle.
Pregnant women need to undergo regular screenings, during which some abnormalities in the development of the heart in the fetus may be detected. When they are detected, the question of the method of delivery is decided.
Other materials on topics:
What should a child's blood pressure be?
Are unvaccinated children the healthiest?
Often – how much? A child who is often ill at a pediatrician's appointment
For reference:
Frolova Tatyana Mikhailovna
Graduate of the pediatric faculty of the Orenburg State Medical Academy in 1997.
From 1997 to 1998 she completed an internship in the specialty “Pediatrics”.
In 2014, she underwent professional retraining in pediatric cardiology, and in 2021 - in functional diagnostics. Candidate of Medical Sciences.
Currently, he is a pediatric cardiologist and functional diagnostics doctor at Clinic Expert, Smolensk. Receives at the address: st. 8 March, no. 20.