© Author: A. Olesya Valerievna, candidate of medical sciences, practicing physician, teacher at a medical university, especially for SosudInfo.ru (about the authors)
Leriche syndrome is a chronic disease in which a narrowing or complete closure of the lumen of the arteries of the legs occurs with impaired circulation. Typically, the pathology is diagnosed in men aged 40-60 years, but in recent years there has been some “rejuvenation” of the group of patients.
The disease is quite dangerous, because it leads to disability in relatively young people, is fraught with fatal complications, and often requires serious surgical treatment. After atherosclerosis of the vessels of the heart and brain, damage to the arteries of the legs takes third place, being detected in almost every fifth patient with atherosclerosis after 50-55 years. In the case of major amputation of a limb, approximately half of the patients are at risk of dying within a year after surgery.
The aorta is the largest vessel in the human body, providing blood to all organs and tissues. In the lower section, it is divided into the right and left iliac arteries, which supply blood to the lower extremities. In Leriche syndrome, the substrate of the disease becomes the lower fragment of the aorta after the renal arteries and iliac vessels depart from it.
Causes
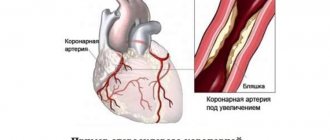
The most common cause of Leriche syndrome is obliterating atherosclerosis of the arteries of the lower extremities. The development of atherosclerosis, in turn, is associated with poor nutrition and bad habits. Against the background of increased levels of cholesterol and its fraction of low-density lipoproteins, cholesterol begins to be deposited in the wall of the arteries. An atherosclerotic plaque gradually forms, which gradually grows and, over time, completely clogs the lumen of the vessel.
Much less often, Leriche syndrome occurs with nonspecific aortoarteritis (inflammatory disease of the arteries of unknown etiology).
Etiology
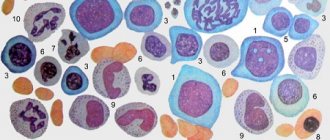
Discussions about the etiology and pathogenesis of Lyell's syndrome continue. The most studied drug form of the disease, which develops due to a violation of the body’s ability to neutralize reactive intermediate drug metabolites. These metabolites interact with tissues, resulting in the formation of an antigenic complex, the immune response to which initiates the development of the disease.
In fact, a genetic predisposition to this pathology has also been proven, in particular in individuals with a number of HLA histological compatibility complex antigens: A2, A29, B12, B27, DR7. The presence of chronic foci of infection in the body (sinusitis, tonsillitis, cholecystitis, etc.), leading to decreased immunity, increases the risk of disease. HIV-infected patients are a special risk group: their risk of developing Lyell's syndrome is 1000 times higher than in the general population.
Symptoms, diagnosis
In Leriche syndrome, the main manifestations are associated with impaired patency of the aorta and its branches, which leads to a deficiency of blood supply to the lower extremities. The main complaint is pain in one or both legs when walking a certain distance (intermittent claudication). Leriche syndrome is characterized by pain when walking not only in the legs, but also in the hips. The more pronounced the narrowing of the arteries, the shorter the pain-free walking distance. Even the degrees of chronic arterial insufficiency are based on the pain-free walking distance.
- 1st degree - more than 500 meters
- 2A degree - from 200 to 500 meters
- 2B degree - from 50 to 200 meters
- 3rd degree - up to 50 meters and pain at rest
- 4th degree - trophic disorders and gangrene
The pulse in the femoral arteries in Leriche syndrome is weakened or absent - this is one of the key symptoms in the clinical diagnosis of this disease.
Other symptoms include chilly feet, decreased muscle mass (hypotrophy) of the lower extremities, and hypotrichosis (hair loss) on the legs. Due to damage to the arteries involved in the blood supply to the cavernous bodies of the penis, impotence may develop.
Of the instrumental diagnostic methods, ultrasound of the arteries plays an important role. The most informative method for diagnosing Leriche syndrome is angiography - the introduction of an X-ray contrast agent into the aorta, followed by a series of X-rays.
From the history of the syndrome
This pathology was first described in 1956 by Scottish dermatologist Alan Lyell. He systematized 11 reports of 14 cases of this disease, 4 of which he personally observed.
Lyell replaced the previously accepted designation “acute pemphigus” with “toxic epidermal necrolysis” (TEN). The fact is that in all patients o. The rash served as the main diagnostic sign for identifying a new nosological unit. Lyell coined the term “toxic” because he believed that the disease was caused by toxemia, a specific toxin circulating in the body. “Necrolysis” is a medical neologism invented by Lyell himself, who combined in it the main clinical sign - “epidermolysis” and the histopathological sign - “necrosis”.
Lyell also noted the severity of damage to the mucous membranes and the unusual weakness of inflammatory processes in the dermis - “dermal silence.”
In the scientific world, the disease received the name of its discoverer during Lyell’s lifetime - in the 60s. However, the dermatologist himself always used the designation TEN.
In 1967, after conducting a targeted survey of colleagues throughout the UK, Lyell presented the most extensive summary of TEN to date - 128 cases of the disease. In the same year, he described 4 forms of TEN, corresponding to a specific etiology: staphylococcal, drug, mixed and idiopathic.
“Necrolysis” is a medical neologism invented by Lyell himself, who combined in it the main clinical sign - “epidermolysis” and the histopathological sign - “necrosis”.
Currently, the staphylococcal form of Lyell's syndrome is identified as a separate nosological unit: staphylococcal scalded skin syndrome (SSSS, L00 according to ICD-10).
Treatment of Leriche syndrome
Conservative therapy includes a diet low in animal fats, taking medications that improve blood supply to the lower extremities (trental, thrombo ACC, rheopolyglucin, actovegin). For high cholesterol levels that do not decrease with diet, drugs that lower cholesterol levels (Torvacard, Crestor) are prescribed.
For severe limb ischemia, surgery is recommended. Most often, prosthetic replacement of the site of the aortic bifurcation is performed, but other interventions are also possible - bypass surgery, endarterectomy, etc. If there is significant concomitant atherosclerotic damage to the distal bed (i.e., arteries of the legs, popliteal arteries), operations may not be indicated.
Treatment
Treatment of Leriche syndrome aims to improve blood flow in the arteries of the legs, prevent the progression of the disease and the development of complications, the most dangerous of which are gangrene, myocardial infarction, and stroke.
Depending on the stage of the disease and the nature of the manifestations, conservative therapy or surgery is prescribed. Conservative treatment includes the prescription of drugs that improve blood circulation in the microvasculature, tissue trophism, and vasodilators.
The patient should know that only treatment prescribed by a doctor will not bring the desired result without excluding risk factors for the disease and lifestyle changes, therefore the main principles of therapy are:
- Elimination of risk factors (control of blood pressure, lipid levels, blood glucose);
- Complete elimination of smoking;
- Regular walks;
- Taking medications to improve blood flow.
Conservative therapy
For stages I and IIA, only conservative treatment is permissible; for more advanced forms, surgery cannot be avoided. Among the drugs prescribed:
- Pentoxifylline, which reduces platelet aggregation and improves the rheological properties of blood. It has been proven that the drug can reduce the symptoms of the disease, but it is effective only in 30-40% of patients;
- Reopoliglucin, reomacrodex, which reduce blood viscosity;
- Acetylsalicylic acid, which prevents thrombosis;
- Cilostazol, which improves blood rheological parameters;
- Ticlopidine, clopidogrel, which have pronounced antiplatelet properties;
- Sulodexide, which reduces viscosity by reducing the content of fats and fibrinogen in the blood;
- Nicotinic acid and its derivatives, which cause dilation of peripheral vessels and promote the breakdown of fibrinogen;
- Antispasmodics (papaverine, drotaverine);
- For severe pain, analgesics are indicated.
For long-term non-healing trophic ulcers, dressings of the affected areas are performed using local agents that improve trophism and regeneration (solcoseryl, methyluracil).
Operation
Surgical treatment is necessary starting from stage IIB of the disease. Before prescribing an operation, the surgeon evaluates the condition of the aorta, vessels of the lower extremities, coronary arteries and cerebral arteries for atherosclerotic lesions and surgical risks associated with it.
For Leriche syndrome, reconstructive operations are performed, the main of which are:
- Endarterectomy – removal of an atherosclerotic plaque with suturing of the vessel or replacement of the defect with synthetic material, native vessels.
- Prosthetics – the altered fragment of the artery is removed, and in its place a synthetic prosthesis or a section of the patient’s vessel taken from another area (autovenous) is installed.
- Aortofemoral bypass surgery - if the lesion is significant, an anastomosis is performed to bypass the damaged area of the vessel (between the aorta and the femoral artery). If the bifurcation of the aorta and both iliac arteries are affected, then a prosthesis is used that completely replaces the site of the bifurcation (in the form of “pants”).
- Stenting – a stent (hollow tube) is installed in a vessel through which blood flows; the method is indicated for patients with damage to the vessels of the heart, brain, or high operational risk when undergoing prosthetics or bypass surgery.
operations for Leriche syndrome – bypass surgery (1) and angioplasty with stenting (2)
If the severity of atherosclerosis is such that it is no longer possible to restore blood flow, or gangrene of the limb has developed, then the only type of operation may be amputation of the leg to a level where blood flow is still present.
It is worth noting that patients who have undergone surgery, as well as those undergoing conservative treatment, must take antiplatelet drugs (aspirin, clopidogrel). In the case of widespread atherosclerosis, such treatment is considered basic and can even be prescribed for life. Vascular drugs are used in courses, and antiplatelet agents are used long-term, throughout life.
Non-drug methods of treating Leriche syndrome consist of ultraviolet and laser irradiation of the blood to reduce its viscosity and reduce platelet aggregation, hyperbaric oxygenation, and physiotherapeutic procedures (UHF, electrophoresis).
Leriche syndrome is a dangerous disease with a serious prognosis. Approximately every third patient who died from cardiovascular pathology has one or another of its manifestations. Prevention of the progression of vascular changes largely depends not only on the timeliness of treatment, but also on the patient’s desire to save the limb and life. Surgeons know of cases where, even after losing a leg, patients did not give up smoking and did not follow the prescribed recommendations. If there are even the slightest signs of impaired arterial blood flow in the vessels of the legs, you should urgently consult a doctor and begin treatment immediately.
Diagnostics
For differential and laboratory diagnosis, provocative tests are not performed, since the risk of uncontrolled complications is high. The most common are extraorganismal diagnostic tests based on the reactions of the patient’s blood cells to a substance that has sensitized the body. These include: the Shelley basophil degranulation test, the Fleck leukocyte agglomeration test, the blast transformation reaction of lymphocytes, hemolytic tests.
HIV-infected patients are 1000 times more likely to develop Lyell's syndrome than the general population.
Apoptosis of keratinocytes is one of the first tissue morphological signs of Lyell's syndrome. Needle biopsy using frozen skin sections is becoming increasingly common. This reveals the absence of typical acantholytic cells, total epidermal necrolysis, sub- and intraepidermal blisters.
Forecast
Since 2011, the SCORTEN scale for assessing the severity of Lyell's syndrome has been widely used in the West. It takes into account the following prognostic factors:
- patient age > 40 years;
- Heart rate > 120 beats. in min.;
- presence of concomitant malignant oncological disease;
- affected body surface area > 10%;
- blood urea level > 10 mmol/l;
- plasma bicarbonate level
- blood glucose > 14 mmol/l.
The presence of each factor increases the risk of death. Thus, the approximate risk of death is: in the presence of 1 factor - up to 3.2%; 2 factors - 12.1%; 3 factors - 35.3%; 4 factors - 58.3%; 5 or more factors – 90%.
Clinical case
In 2009, in Donetsk, I witnessed a rare case for Donbass (only 6 cases in the Donetsk region from 1991 to 2013!) case of Lyell's syndrome.
Patient: 37 years old. Allergic and infectious anamnesis are not burdened. Three days before admission, she fell ill with a cold. She was treated with “familiar” medications: cough tablets, eye drops, nasal drops, vitamins. From the evening of the second day, itching and rashes appeared. She took suprastin on her own. After short-term relief, the condition worsened. In the evening on the third day, after fainting, she was taken to the city hospital by emergency medical services, and within a few hours was transferred to a regional clinic. A woman was admitted with hyperemic skin on her chest, shoulders, and inner thighs. On the third day, bubbles filled with cloudy contents appeared. The volume of others reached 100 ml. Throughout the entire period, hyperemia of the eyelids, sclera, mucous membranes of the oral cavity, and perianal area persisted.
From the third day, the combustiologist made repeated attempts to close the wound surface of the xenoskin. However, short-term periods of calm were replaced by psychomotor agitation in the patient, which led to displacement of the bandages and xenoskin. Not a single flap took root. Over the course of two weeks in the intensive care unit, the patient spent more than half of the time in forced medicated sleep. And from the sixth day, when the patient’s condition became critical, she was transferred to permanent mechanical ventilation.
In this case, Lyell's syndrome was diagnosed within two days after the patient was admitted to the hospital; the course of the disease was not lightning fast, but rather acute; Asymptomatic therapy was carried out, but it was not possible to save the woman.
Flow
Based on the nature of the course, there are three variants of the clinical picture of Lyell’s syndrome:
- Fulminant form - up to 10% of all cases. Develops over several hours. Etiology: idiopathic or drug-induced. Skin lesions cover up to 90% of the body surface per day. Impaired consciousness up to coma. Acute renal failure - anuria. Due to the fact that most of these patients do not survive to hospitalization or are admitted in a terminal condition, the fatal outcome is 95% within 2–3 days. At autopsy, the internal organs are usually intact.
- Acute form - 50–60% of cases. Damage to the skin and mucous membranes goes through the entire spectrum of maturation: from rashes to necrolysis. The area of necrolyzed surfaces can reach 70% of the body surface. The disease lasts from 7 to 20 days. Starting from 3–4 days, symptoms of renal, hepatic, cardiovascular, and pulmonary failure appear, as well as infectious complications—primarily pulmonary and genitourinary system infections—and as the disease progresses, sepsis. Mortality reaches 60%.
- Favorable course (smoothed form) - frequency up to 30% of cases. Damage to the skin and mucous membranes does not exceed 50% of the body surface. Clinical manifestations reach their peak on days 5–6 of the disease. Then, within 3–6 weeks, the patient’s condition improves until full health is restored.
The overwhelming majority of patients - more than 90% - have erosive changes in the mucous membranes. Typical complaints are pain along the urethra during urination and photophobia.
A positive Nikolsky symptom is characteristic: detachment of the epidermis on externally unchanged skin with sliding pressure and detachment of the peri-vesical epidermis when pulling on a piece of the vesical tire. In especially severe forms, total detachment of the epidermis is observed due to friction over the entire surface of the patient’s body.