Transposition of the great vessels
Transposition of the great vessels (TMS) means the incorrect position of the main vessels leaving the heart, i.e. the aorta and the trunk of the pulmonary artery, relative to each other and relative to the chambers of the heart from which they arise.
There can be many options for transposition: complete, incomplete, corrected, in combination with other defects.
For now we will only touch on the full
transpositions, i.e.
situations when the vessels have completely moved and changed their places. The aorta arises from the right ventricle, and the pulmonary artery arises from the left. The remaining parts of the heart, i.e. the atria with the veins flowing into them, and the ventricles, are normal and do not have any other defects (the term “simple TMS” is sometimes used). It’s not hard to imagine, but this happens to the heart, and not so rarely. It’s as if legs grew where arms should be, and arms grew where legs should be. Fortunately, it doesn't look that scary. Children are born full-term, completely normal, but, unlike tetralogy of Fallot, they are immediately very cyanotic. It becomes obvious that immediately after birth it is very difficult for a child to simply live
.
Venous blood, poor in oxygen, enters the right atrium, the right ventricle, and from here again into the aorta departing from it and into the systemic circulation, without passing through the lungs, without being saturated with oxygen and without giving off carbon dioxide. And blood from the lungs through the pulmonary veins goes to the left atrium, to the left ventricle, and again to the pulmonary artery and to the lungs, which from the point of view of its saturation with oxygen is meaningless, because she is already saturated. Two separate circles of blood circulation are formed.
And, if we previously conventionally depicted the relationship of the circulatory circles in the form of a figure eight lying on its side, then with transposition these are two closed rings not connected to each other.
It is clear that this state of affairs is simply incompatible with life. But nature decides in its own way: it leaves open the oval window (i.e., a natural defect) in the interatrial septum, through which part of the venous blood leaks into the left sections, and then into the lungs. Both circles are connected to each other only by this shunt.
It is clear that the amount of blood that passes through the defect with each cardiac cycle, and on which its saturation depends, is very small and cannot in any way meet the body’s needs. If there are two defects, or a defect of the interventricular septum is added, then this is somewhat better, because the amount of oxidized blood in the arterial system becomes greater. But still it is extremely insufficient.
Children born with complete transposition of the great vessels quickly fall into a critical condition, and if they are not helped in the first days of life, they will die. They will not have attacks of shortness of breath, as with tetralogy of Fallot, but cyanosis appears already in the first hours, and the slightest physical effort - movements, sucking, crying - becomes difficult or completely impossible. What needs to be done? First of all, expand the existing defect, increase its size in order to increase the volume of venous blood passing through it.
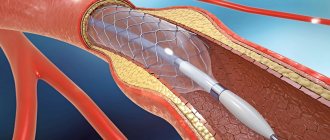
This is achieved by the so-called Rashkind procedure, the essence of which boils down to the fact that a catheter with a balloon is inserted into the open oval window, which is inflated, thereby rupturing the interatrial septum and increasing the defect in diameter. The procedure is performed in the X-ray surgery room and preparation for it includes all the points that we described above when we talked about cardiac catheterization or closure of the patent ductus arteriosus.
In case of complete transposition, expansion of the defect must be done urgently. But this expansion - and the increase in the flow of mixed blood - in itself does not solve anything. It only slightly improves the child’s condition and prolongs his life, and something needs to be done further without delay. The effect of the procedure will be very short-lived - only a few weeks, and if you wait longer, the child may die from heart failure and constant oxygen starvation.
It is clear that the ideal method of treating transposition is the complete elimination of this “error of nature” - i.e. surgical relocation of the aorta and connecting it to “its” left ventricle (whereas it now departs from the right), and the pulmonary artery to the right ventricle.
Description of the operation of surgical relocation of the aorta and connecting it to “one’s” left ventricle
After the usual introduction of the child into anesthesia, opening the chest, connecting to the apparatus, artificial circulation is started, with the help of which the blood is simultaneously cooled (this is always done during other operations that may require quite a long time - 1.5-2 hours or more) . The fact is that when cooling, all metabolic processes slow down (like a bear in hibernation), and this protects the body from all sorts of complications in the future. With the help of the device, cooling occurs quickly (as does warming in the final stage of the operation).
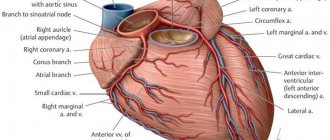
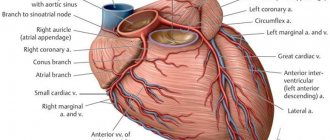
The aorta and pulmonary artery are divided in half. The coronary arteries are cut off from the aorta and sutured into the beginning of the pulmonary artery, which will then become the mouth of the new aorta. The cut off “own” aorta is sutured to this area, and then a tube is made from a piece of its own pericardium, which is sewn into the new pulmonary artery, restoring it too.
Thus, true anatomical correction of the defect is achieved. Now everything is fine: the great vessels depart from the ventricles from which they should depart. This operation, as we see, is complex and lengthy. But today it is done quite successfully in several cardiology clinics in the country. However, to count on success, it must be done very early, i.e. in the first weeks of life.
The fact is that at birth both ventricles, right and left, are well developed, have the same muscle mass and wall thickness. With normal development in the right
the load of the ventricle is less than that of the left: it does not need to pump blood into a large circle, i.e.
all over his body, and he gets used to it pretty quickly. A little time will pass - and its wall will become thinner, and the muscle mass will decrease: why work if you don’t have to work? The same thing happens with transposition - but with the left
ventricle.
During transposition, the ventricles of the newborn are also initially identical, and the fact that they work against different resistances of the systemic and pulmonary circulation does not affect them at first. But then the left ventricle becomes thinner and loses mass, but after the operation of moving the vessels, it is he who will have to do the main work. And here it is important not to waste time, because... If you wait several months, then even if the Rashkind procedure has a good effect, radical correction will no longer be possible. The best time for such a correction is the first month of life
.
It must be said that this treatment of complete transposition has been used for 25 years, and in recent years it has become standard. It is clear that to successfully perform this complex operation, not only a well-developed technique is required, but also methods of providing anesthesia, artificial circulation, and management of the postoperative period that are safe for the infant, i.e. everything that leads to ultimate success. This can only be done in large pediatric cardiac surgery centers with extensive experience in treating congenital heart defects.
What to expect after surgery? Overall, the results are very good. Today, hundreds of operated patients lead normal lives, and the life expectancy of some children who were among the first to be operated on is already 20 years or more. Of course, observation by a cardiologist, and sometimes detailed examinations, are mandatory, because As the child and the heart itself grow, problems may arise. However, the main of these problems can be completely eliminated by X-ray surgery, without resorting to repeated surgery.
Unfortunately, radical surgery is not always possible. The main reason is late contact with specialists, when time has already been lost. It is not uncommon to see children with complete transposition at the age of one or two years. They are very blue and are greatly retarded in physical development. Their eyes—intelligent, suffering, and seemingly understanding everything—can never be forgotten. These children can and should also be helped urgently, and such methods exist, they have been used for a long time, and they have proven themselves well. Long before surgical science made possible early and anatomically radical treatment of transposition, another, less radical, but quite effective method was proposed.
The idea is not to correct the anatomy (this was technically impossible then), but to change the paths of blood flow, i.e. the direction of blood from the veins to the lungs, to the pulmonary circle, and the oxidized blood to the left ventricle and the aorta, i.e. in a big circle.
Techniques known as " intra-atrial correction"
“were for a long time the only ones in the treatment of transposition, but they are still used today when, for some reason, it is not possible to perform anatomical correction.
The essence of the operation comes down to dissecting the right atrium, removing the entire interatrial septum and sewing a patch inside the cavity from the child’s own tissues (pericardium, or the wall of the atrium) in such a way that blood from the vena cava is directed to the left ventricle, from which the pulmonary artery arises, and then - into the lungs, and from the pulmonary veins into the right ventricle, into the aorta and into the systemic circulation. These operations, known by the names of their authors - Mustard and Senning, correct hemodynamics, but not the defect itself. Today, the world has accumulated a great deal of experience in such operations, and the fate of the operated patients has been tracked for several decades. Half of them have a normal, fairly active and long life. Over time, the other part may experience complications in the form of rhythm disturbances, insufficiency of atrioventricular valves - after all, the ventricles of the heart remain in place and do not work as intended by nature. People who have had this type of surgery sometimes feel a little blue—especially their lips and fingernails and toenails. There are still restrictions on physical activity. Girls who have reached adulthood may not be recommended to have children, not because the child will have a defect - this is a complete misconception, but because pregnancy and childbirth may be too much physical exertion. But, be that as it may, intra-atrial correction methods saved the lives of hundreds of children. So, even if the moment for anatomical correction is missed, there is a way out, and a good way out.
Moreover, in recent years, operations have begun to move vessels with the removal of old intra-atrial patches. This is not always possible and necessary, and it cannot be called anything other than “aerobatics” in cardiac surgery. But time moves forward, and I just want you to believe: transposition of the great vessels today is a completely curable defect, and not a single child born with it should die. But at the same time, its future depends largely on you and on your faith in the modern possibilities of medicine.
How to get treatment at the Scientific Center named after. A.N. Bakuleva?
Online consultations
Causes of TMS
The exact reasons for the appearance of pathology in a particular baby are usually impossible to establish, because the mother could have been exposed to a variety of adverse effects during pregnancy. The following may play a role in the occurrence of this anomaly:
- Viral diseases during pregnancy (rubella, chickenpox, herpes, respiratory infections);
- Severe gestosis;
- Ionizing radiation;
- Consumption of alcohol, drugs with teratogenic or mutagenic effects;
- Concomitant pathology in a pregnant woman (diabetes, for example);
- The mother is over 35 years old, especially if this is the first pregnancy.
It has been noted that TMS occurs more often in children with Down syndrome, the causes of which are chromosomal abnormalities caused by the reasons listed above, among others. Children with TMS may also be diagnosed with defects of other organs.
There may be an influence of heredity, although the exact gene responsible for abnormal heart development has not yet been found. In some cases, the cause is a spontaneous mutation, while the mother denies the possibility of external influence in the form of x-rays, drugs or infections.
The formation of organs and systems occurs in the first two months of embryo development, so during this period it is necessary to protect the very sensitive embryo from all kinds of toxic factors. If the heart begins to form incorrectly, then it will not change, and signs of the defect will appear immediately after birth.
Prognosis and treatment results
When a baby is born with transposition of blood vessels, his parents are very concerned about not only the operation, but also what will happen after, how the child will develop and what awaits him in the future. With timely surgical treatment, the prognosis is quite favorable: up to 90% or more of patients live a normal life, periodically visiting a cardiologist and undergoing a minimum of examinations to monitor the functioning of the organ.
With complex defects, the situation may be worse, but most patients still have an acceptable quality of life. After intra-atrial correction surgery, about half of the patients do not experience restrictions in life, and its duration is quite long. The other half may suffer from arrhythmias and heart failure, which is why it is recommended to limit physical activity, and women are warned about the risks during pregnancy and childbirth.
Today, TMS is a completely curable anomaly, and hundreds of children and adults who have successfully undergone surgery are proof of this. Much depends on the parents, their faith in success and desire to help their baby.
Manifestations of TMS
During intrauterine development, this heart defect does not manifest itself in any way, because in the fetus the pulmonary circle does not work. After birth, when the baby’s heart begins to pump blood to the lungs on its own, TMS also manifests itself in full. If the transposition is corrected, then the clinical picture is poor; if the defect is complete, its signs will not be long in coming.
The degree of impairment with complete TMS depends on the communication pathways and their size. The more blood mixes in the heart in newborns, the more oxygen the tissues will receive. The optimal option is when there are sufficient holes in the septa, and the pulmonary artery is somewhat narrowed, which prevents volume overload of the pulmonary circle. Complete transposition without additional anomalies is incompatible with life.
Babies with transposition of the main vessels are born at term, with normal weight or even large, and already in the first hours of life signs of congenital heart disease are noticeable:
- Severe cyanosis of the whole body;
- Dyspnea;
- Increased heart rate.
Further, the symptoms of heart failure rapidly increase:
- The heart increases in size;
- Fluid appears in the cavities (ascites, hydrothorax);
- The liver enlarges;
- Swelling occurs.
Other signs of cardiac dysfunction are also noteworthy. The so-called “heart hump” (deformation of the chest) is caused by an enlargement of the heart, the nail phalanges of the fingers thicken, the baby lags behind in development, and does not gain weight well. Certain difficulties arise during feeding, since it is difficult for a child to suckle at the breast with severe shortness of breath. Any movement and even crying can be an impossible task for such a baby.
If an excess amount of blood enters the lungs, there is a tendency to infectious and inflammatory processes and frequent pneumonia.
The corrected form of TMS proceeds much more favorably. In the absence of other cardiac defects, clinical transposition may not occur at all, because the blood moves correctly. The child will grow and develop correctly according to his age, and the defect can be detected accidentally by the presence of tachycardia, heart murmur, or conduction disturbances.
If the corrected transposition is combined with other disorders, then the symptoms will be determined by them. For example, if there is a hole in the interventricular septum, shortness of breath will appear, the pulse will increase, and signs of heart failure will appear in the form of edema and enlarged liver. Such children suffer from pneumonia.
Classification
Depending on the accompanying defects that perform the role of shunts compensating for hemodynamics during TMS, a number of variants of this anomaly of the heart and blood vessels are distinguished:
- a defect accompanied by a sufficient volume of pulmonary blood flow and hypervolemia and combined with a patent foramen ovale (or simple TMS), a ventricular septal defect or a patent ductus arteriosus and the presence of additional shunts;
- a defect accompanied by insufficient pulmonary blood flow and combined with a ventricular septal defect and stenosis of the outflow tract (complex TMS) or with a narrowing of the outflow tract of the left ventricle.
In approximately 90% of patients, TMS is combined with hypervolemia of the pulmonary circulation. In addition, 80% of patients have one or more additional compensating shunts.
The most favorable option for TMS is in cases where, due to defects of the interatrial and interventricular septa, sufficient mixing of arterial and venous blood is ensured, and moderate narrowing of the pulmonary artery prevents the onset of significant pulmonary hypervolemia.
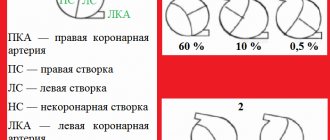
Normally, the aorta and pulmonary trunk are in a crossed state. During transposition, these vessels are located parallel. Depending on their relative position, the following TMS options are distinguished:
- D-option – aorta to the right of the pulmonary trunk (in 60% of cases);
- L-variant – aorta to the left of the pulmonary trunk (in 40% of cases).
Diagnostics
In almost 100% of cases, this heart defect is diagnosed immediately after the birth of a child, in the maternity hospital.
Most often, TMS is detected in the maternity hospital. When examining the child, the doctor detects a pronounced medially displaced cardiac impulse, cardiac hyperactivity, cyanosis and expansion of the chest. When listening to the sounds, an increase in both tones, the presence of systolic murmur and murmurs characteristic of concomitant cardiac defects are revealed.
For a detailed examination of a child with TMS, the following diagnostic methods are prescribed:
- ECG;
- Echo-CG;
- chest x-ray;
- catheterization of cardiac cavities;
- angiocardiography (aorto-, atrio-, ventriculo- and coronary angiography).
Based on the results of instrumental studies of the heart, the cardiac surgeon draws up a plan for further surgical correction of the anomaly.