Aortic regurgitation refers to a heart defect in which damage to the aortic valve prevents the semilunar valves from closing completely. This causes a characteristic circulatory disorder. When the heart contracts, blood is ejected from the left ventricle and then flows through the aorta into other vessels. In the absence of pathology in this area, the aortic valve flaps are completely connected, and this prevents blood from returning back. Blood moves through the aorta, completing its circulation. But if a pathology such as aortic valve insufficiency develops, normal blood flow is disrupted, the aortic valves do not completely close the aortic opening and part of the blood returns back to the left ventricle. Blood from the left atrium also arrives at the same time. There is much more blood in the left ventricle than it should be, it becomes overfilled, it rises, it needs to cope with a large volume of blood, making great efforts to maintain blood flow. Over time, as a result of this increased load, the muscle that pushes blood out becomes thicker. In addition, against the background of aortic insufficiency, the heart itself does not receive sufficient nutrition due to impaired coronary blood flow. This further aggravates the heart condition. Aortic valve insufficiency can be an isolated defect, or it can occur in various forms with other heart defects.
Symptoms
Given the large compensatory capabilities of the myocardium, the disease can be asymptomatic for a long time. And even when doing physical exercise, a person may not immediately feel any symptoms. Further progression of coronary and cerebral disorders lead to the appearance of the first symptoms in the form of dizziness, weakness, fatigue, increased heart rate and increased heart rate. Aortic insufficiency is manifested by tachycardia, felt at rest, symptoms intensify after physical exertion. There is pallor. Shortness of breath and angina attacks develop, which are poorly relieved by nitroglycerin.
A person with aortic valve insufficiency has external characteristic manifestations. He can see the pulsation of the cervical vessels “carotid dance” and he shakes his head in time with the pulse. When measuring blood pressure, increased systolic pressure is detected, but diastolic pressure always decreases, sometimes down to zero. Blood pressure always changes. The pulse is fast, high, large. An intensified elevating apical impulse is detected. The heart expands to the left.
When listening, there is a weakening of the first tone at the apex, and a weakening of the second tone above the aorta (with severe destruction of the valve leaflets - until it completely disappears). A soft blowing diastolic murmur appears in the third intercostal space on the left and above the aorta. It can be heard more clearly if the patient exhales completely and holds his breath. Changes in blood flow that occur against the background of this defect cause a large expansion of the left ventricle, leading to mitral valve insufficiency. This will be manifested by the appearance of a systolic murmur. It is heard at the apex of the heart. Less common is Flint's diastolic murmur. Sometimes with this defect you can hear two noises on the femoral artery.
Types and stages
For aortic regurgitation, doctors use a classification based on the severity of regurgitation (backflow of blood). the degree is determined only by a functional diagnostics doctor based on the results of echocardiography:
- Soft (light);
- Moderate;
- Expressed.
There are many ways to define it. But all of them are possible thanks to Doppler research. All echocardiography devices have this function. It allows you to detect pathological flows inside the heart using an ultrasound sensor. One way or another, this is the most objective assessment of the severity of aortic insufficiency.
Acute and chronic deficiency are also distinguished. This is largely a clinical classification based on symptoms and how quickly they develop.
Diagnostics
First of all, the doctor can think about the presence of aortic valve insufficiency based on the results of the examination of the patient. Because the manifestations of this pathology have their own characteristics, revealed externally and by listening. As mentioned above, at a certain stage in the development of the disease, the patient’s characteristic appearance appears and heart murmurs appear. The diagnosis is confirmed after special research methods. Echocardiography can detect signs of this defect in the form of reverse blood flow, increased work of the muscular wall of the left ventricle in systole, and fluttering of the mitral valve as blood fills the left ventricle. A phonocardiogram clearly reveals changes in tones and noises that identify this defect. ECG and x-ray of the heart may not detect changes for a long time. They are detected already in the later stages, when left ventricular hypertrophy develops.
Causes and risk factors
Aortic valve insufficiency develops due to loose closure of the valves during the relaxation phase of the ventricles, which can develop for a number of reasons:
- idiopathic (unknown cause) dilation of the aorta;
- congenital defects of the aortic valve (usually bicuspid aortic valve);
- sclerosis of the valves (due to atherosclerosis);
- rheumatism;
- infective endocarditis;
- arterial hypertension;
- myxomatous degeneration (disorder of connective tissue development);
- dissection of the ascending aorta;
- Marfan syndrome;
- aortic valve injuries;
- ankylosing spondylitis;
- syphilitic aortitis;
- rheumatoid arthritis.
Most of these causes lead to chronic aortic insufficiency, which can be asymptomatic for a long time. Others, in particular infective endocarditis, aortic dissection, and trauma are often accompanied by a sudden development of severe aortic insufficiency. This leads to serious hemodynamic disturbances. As a result, much less blood reaches vital organs: the brain, kidneys, liver, heart.
Treatment of aortic valve insufficiency
There are two types of treatment for this pathology. Aortic insufficiency is eliminated if treated with surgery, which radically solves the problem. In this case, an artificial valve is implanted. But the positive outcome of such an operation depends on the severity of the changes that have occurred in the myocardium.
Aortic valve insufficiency is treated conservatively; treatment is aimed at reducing the symptoms of this disease, which can be eliminated temporarily. At the same time, the time of onset of heart failure is delayed. The conservative method is aimed at maintaining the functioning of the heart and improving the condition of other organs. In order to prevent cerebral circulatory failure, as well as coronary circulatory failure, it is necessary to maintain a sufficient heart rate. This becomes possible with the use of cardiac glycosides (korglykon, strophanthin and others).
Vitamins, cocarboxylase, and riboxin are also used to maintain nutrition of the heart muscle. If complications occur, their treatment is prescribed.
Aortic insufficiency
Aortic insufficiency is a dysfunction of the aortic valve, in which the valves do not close completely and blood returns from the main vessel of the body - the aorta - back to the heart.
What is aortic insufficiency?
Aortic insufficiency can be congenital (due to impaired formation of the aortic valve during intrauterine development) and acquired (due to the effects of pathological processes, that is, diseases).
Why does it arise?
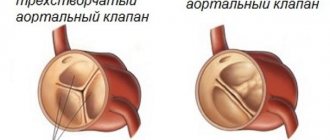
Normally, the aortic valve has 3 thin cusps, which, when opening, allow blood from the heart to the internal organs, and when closing, prevent blood from getting back into the heart and overloading it.
Quite often, as a result of a violation of intrauterine development, the aortic valve from birth may have only 2 leaflets, this leads to accelerated “aging” of the valve with the formation of a narrowing of its lumen and/or unevenness of the leaflets.
The second common cause of aortic insufficiency is infective endocarditis. This extremely dangerous disease is characterized by inflammation and destruction of vital structures of the heart with the formation of heart failure and vegetations (accumulations of colonies of microorganisms on destroyed heart structures). An absolutely healthy person can develop infective endocarditis against the background of complete well-being. It is worth noting that aortic valves with congenital malformations are most often affected by infection.
Everyone knows such a disease as atherosclerosis; it affects the vessels of all organs, as well as some structures of the heart. The aortic valve is an intravascular formation as it is located in the lumen of the main artery of the body, the aorta. When atherosclerotic plaques develop on the aortic valve, thickening of the leaflets may occur. Thickened valves lose elasticity and become covered with calcium salts, which leads to disruption of closure and backflow of blood.
Who can get sick
The disease is typical for patients of any age. Children are born with a bicuspid aortic valve, which makes them sick from birth; often the disease is detected when a dangerous complication occurs - infective endocarditis or dissection (dissection) of the aorta. ( Any age )
Atherosclerosis progresses with age in all people, causing the gradual formation of aortic insufficiency in a certain proportion of the population. ( Most typically from 45 to 70 years old )
A special group consists of patients with infective endocarditis. ( Any age )
What are the symptoms of the disease?
Aortic insufficiency is a disease in which no symptoms at all may occur for a long time; this is due to the compensatory capabilities of the body. In acute aortic insufficiency, symptoms appear at lightning speed and often lead to death in the first days of the disease.
The following complaints are typical for this disease:
- Shortness of breath during moderate physical activity (people around you may notice that you get tired more quickly)
- Palpitations, sensation of heart pulsation in the left side of the chest
- Interruptions in heart function
- Feeling of pulsation in the vessels of the whole body, head, fingertips. The pulsation of the vessels of the neck is especially noticeable.
- Dizziness when changing body position, or physical effort, stress.
- Late stages of the disease are characterized by sudden attacks of loss of consciousness
- Edema of the lower extremities
How is the diagnosis made?
Most often, when undergoing a professional examination, medical examination, or fluorography, doctors may notice significant deviations in the shape of the heart or changes in the electrocardiogram. An experienced cardiologist will always be able to hear a heart murmur characteristic of aortic insufficiency and will prescribe a number of studies:
- Electrocardiograms
- X-ray of the chest organs
- ECHO-cardiography (ultrasound of the heart)
- In difficult cases, multislice computed tomography with the introduction of a contrast agent is required.
This scope of research allows you to confirm or exclude the diagnosis, determine the stage of the disease and prognosis.
What are the stages of the disease?
Aortic insufficiency occurs:
- Easy
- Moderate
- Expressed
- Heavy
Who is treating?
It all depends on the cause, severity and presence of symptoms. Mild to moderate aortic insufficiency, not associated with infective endocarditis, and not accompanied by symptoms of heart failure, is observed by a cardiologist with periodic consultations with a cardiac surgeon.
If there are signs of infective endocarditis, treatment is carried out by a cardiac surgeon, regardless of the degree of damage and the presence of symptoms. Severe aortic insufficiency is treated by a cardiac surgeon. Treatment method: surgical replacement of the aortic valve, plastic surgery of the aortic valve, replacement of the ascending aorta.
What are the approaches to surgical treatment?
Depending on the stage of the disease, the patient’s age and many other factors, there are open surgical techniques and minimally invasive methods.
Each method has its own advantages and disadvantages.
Aortic valve replacement using an open technique under artificial circulation.
During open surgery, a longitudinal incision of the sternum and complete visualization of the heart are performed under artificial circulation. Then a heart-lung machine is connected, the heart stops, the altered heart valve is excised, and a prosthetic heart valve is securely sewn in its place.
Advantages of the method:
- Wide use
- This approach is considered excellent
- It is easy to influence complications that arise during surgery
Disadvantages of the method:
- Significant surgical trauma (scar length 20-25 cm).
- The need to sleep strictly on your back for 3 to 6 months.
Duration of the operation: from 3 to 6 hours.
In the intensive care unit: usually about 36 hours.
Total duration of hospitalization: 12-15 days.
Risk of intervention: about 1.5%
Aortic valve replacement from a mini-access under artificial circulation
This surgical correction option is characterized by a smaller incision, which is less traumatic for the patient. The course of the operation is similar to open surgery.
Advantages of the method:
- Less traumatic method
- Cut about 10 cm long
- Early rehabilitation
- There is no need to sleep on your back for long periods of time
Disadvantages of the method:
- Great technical complexity
- Limited ability to influence complications during surgery, or requires switching to a larger incision
Duration of the operation: from 2 to 8 hours.
In the intensive care unit: usually about 24 hours.
Total duration of hospitalization: 10-15 days.
Risk of intervention: more than 2%
Aortic valve plastic surgery
In rare cases in adults and quite often in children, the valve can be preserved by modifying its weak points surgically.
Advantages of the method:
- There is no need for lifelong use of anticoagulants, you continue to live with your own valve
Disadvantages of the method:
- It is difficult to predict the duration of the effective correction period
- Repeat surgery may be required if the valve ruptures again
Duration of the operation: from 3 to 8 hours.
In the intensive care unit: usually about 36 hours.
Total duration of hospitalization: 12-15 days.
Risk of intervention: moderate
What's the prognosis?
If you seek medical help in a timely manner, most patients, after successful surgical treatment, fully return to normal life within 3-6 months. People who work physically can return to work after 4-6 months; if the work does not involve physical effort, 6-8 weeks is often enough for rehabilitation. It should be understood that in each specific case the pace of rehabilitation is individual and depends on the patient’s age, the degree of “neglect” of the case, the presence of concomitant diseases, and complications during treatment.
I need to get examined! What are the stages?
1. Consultation with a cardiac surgeon.
After an in-person examination and a standard physical examination, it is possible with a high degree of probability to confirm or refute aortic stenosis.
Research will be conducted:
- Electrocardiography
- ECHO-cardiography (ultrasound of the heart)
If the diagnosis is confirmed, further examination is indicated before hospitalization in a specialized hospital.
- Determination of blood group, Rh factor
- Diagnosis of HIV, hepatitis B, C, syphilis
- General urine analysis
- General blood analysis
- Standard biochemical blood test
- X-ray of the chest organs, or fluorography
- Consultation with a urologist for men, a gynecologist for women
- Fibrogastroscopy
The main purpose of the examination before planned hospitalization is to exclude possible contraindications.
2. Hospitalization to a specialized hospital for further examination
In a hospital setting the following will be performed:
- Coronary angiography (men over 40 years old, women in menopause)
- Control ECHO-cardiography
- Examination with the participation of the head of the department or a professor as part of a council in order to determine the indications for surgical treatment and the choice of treatment tactics.
3. Discharge from the hospital with the exact date of hospitalization for surgical treatment if consent and indications are available.
4. Registration of a quota of high-tech medical care for surgical intervention.
5. Hospitalization for surgical treatment
6. Postoperative observation.
If you find yourself with similar symptoms, or your cardiologist suggests this diagnosis, do not hesitate, seek qualified medical help, we will conduct an examination on an outpatient basis, accompany hospitalization in a specialized hospital for high-tech additional examination and surgical treatment, and ensure proper monitoring after the operation.
Without surgical treatment of severe forms, the long-term prognosis for life is unfavorable. Patients die from acute myocardial infarction, sudden arrhythmic death, rupture of aortic aneurysm, aortic dissection, and progressive congestive heart failure.
Remember: aortic valve insufficiency is a structural change in the heart, cannot be cured by any drug, and if the cause is infective endocarditis, emergency surgery is often required!!!
Make an appointment now
Anatomical features of the pathology
In order to understand an anomaly, you need to have an idea of the norm. The aortic valve is an anatomical formation that is located at the junction of the left ventricle of the heart into the aorta.
Normally, it consists of three valves that close and open to perform their function. The valve's job is to allow blood to pass from the heart cavity into the aorta, from where it is distributed throughout the body. Functionally, it is a kind of tightly closed door that opens only at the right moment.
Due to these reasons, the aortic valve may develop incorrectly and end up with two leaflets instead of three. Most often, developmental disorders occur between the 3rd and 8th weeks of intrauterine development of the unborn child. This anomaly can occur in combination with other congenital heart defects, and is most often inherited in an autosomal dominant manner.
One of the options for classifying mechanical phenotypes of DAK valves
There are 2 options for abnormal intrauterine development of the aortic valve (the numbering coincides with that shown in the figure above):
- One leaf is complete, and the other two are fused together.
- There are only two doors. This option is more dangerous, because a strong load is placed on the valves, the valve wears out very quickly and blood flows back.
Both cases occur with approximately equal frequency among patients. But in the future, in any case, they lead to various kinds of complications.
In patients with a 2-leaf aortic valve, not only the speed of blood flow is impaired, but also a pathological level of tension in the walls of the aorta at its mouth is determined. The blood flow becomes turbulent (fast, restless).
Because of this, aneurysms may occur in the future - bulging of individual sections of the vessel, leading to its rupture. In any case, congenital heart disease (bicuspid aortic valve) leads to various cardiac complications, which can go unnoticed for a long time.
Diagnosis of arterial insufficiency
First, an external examination of the patient is carried out, especially paying attention to the color of the skin of the limbs and around the lips, then the patient’s heart is listened to and an anamnesis is taken. To accurately diagnose arterial valve insufficiency, the following methods are used: - radiography (diagnosis of changes in the lungs); — electrocardiography (registration of heart biorhythms); - phonocardiography (determine the characteristics of systolic murmurs); — sounding (insertion of a catheter into the heart to take samples); — echocardiography (determine structural pathologies of the heart muscle); - ventriculography (helps to evaluate the structure of the cavities of the heart, its contractility, to identify various possible defects...).
Forecast
The prognosis for aortic insufficiency is better, the lower the degree of regurgitation and the earlier treatment is started. Preventive examination by a general practitioner, cardiologist, full antibiotic therapy in case of infective endocarditis and rheumatic fever - all this helps to improve the prognosis. It is very important to listen to yourself, your body, so as not to miss the first symptoms (lethargy, decreased performance, fainting, shortness of breath during physical activity).
Usually, with severe clinical heart failure, the prognosis worsens, since irreversible changes occur in the structure of the heart.
Diagnostic tests
Common tests to diagnose aortic valve regurgitation include:
- Echocardiogram.
This test uses sound waves to produce an image of your heart. In echocardiography, sound waves are sent to your heart from a wand-like device (transducer) placed on your chest. Sound waves bounce off your heart and are reflected back through your chest wall and processed electronically to provide video images of your heart. An echocardiogram allows your doctor to take a close look at your aortic valve. A certain type of echocardiography, Doppler echocardiography, may be used. This allows measurements of the volume of blood that flows in the opposite direction through the aortic valve. This volume is expressed in cubic centimeters per beat. - Chest X-ray.
Using a chest X-ray, your doctor can examine the shape and size of your heart to determine whether your left ventricle is enlarged, a possible sign of damage to the aortic valve. - Electrocardiogram (ECG).
In this test, wires (electrodes) are attached to your skin to measure electrical impulses from your heart. The pulses are reflected as waves displayed on a monitor or printed on paper. An ECG can provide information about whether the left ventricle is enlarged, a problem that can occur with aortic valve insufficiency. - Transesophageal echocardiography.
This type of echocardiography allows you to take a closer look at your aortic valve. A “sensor tube” is inserted through your esophagus and goes into your stomach and is closer to your heart. In traditional echocardiography, a device called a transducer moves on your chest to produce the sound waves needed to create a picture of your beating heart. In transesophageal echocardiography, a small probe is attached to the end of a tube and passed through the esophagus. This is done to better visualize the image of your aortic valve and the bleeding through it, since the sensor is closer to the valve itself. - Exercises, tests.
Various types of exercise tests to assess activity tolerance and test your heart's response to exercise (sports). - Cardiac catheterization.
Your doctor may order this procedure if noninvasive tests have not provided enough information to firmly diagnose the type and severity of your heart disease. The doctor threads a thin tube (catheter) through a blood vessel in your arm or groin and into your heart. A contrast agent is injected through a catheter in your heart, making details visible on an X-ray. Cardiac catheterization can show if blood is flowing back from the aorta in the heart into the left ventricle. Some catheters are equipped with special sensors that can measure pressure within the chambers of the heart. Pressure may be increased in the left ventricle with aortic valve insufficiency.
ECG
These tests help doctors diagnose aortic valve regurgitation, determine how severe the problem is, and decide whether your aortic valve needs replacement.
Treatment
Aortic insufficiency is treated by a cardiologist and cardiovascular surgeon.
Drug treatment
Drug treatment is prescribed depending on the cause of aortic insufficiency. It is considered as an option in preparation for surgery or to reduce the symptoms of heart failure and alleviate the condition of patients who have contraindications to surgical treatment.
For rheumatism and infective endocarditis, a course of antibacterial therapy is prescribed. In the first case, penicillin antibiotics (benzathine benzylpenicillin) are used to prevent exacerbation of the disease. For infective endocarditis, amoxicillin, ceftriaxone, gentamicin, and, less commonly, vancomycin are usually prescribed for a long course of 2 weeks. Drugs are prescribed based on the clinic and the resistance of bacteria to them. Can be used as a single drug or in combination.
Treatment of arterial hypertension consists of prescribing ACE inhibitors (perindopril, enalapril, lisinopril) or sartans (valsartan, losartan) and dihydropyridine calcium antagonists (nifedipine, amlodipine).
Beta blockers (bisoprolol, metoprolol, nebivolol) are added to treatment in the case of reduced cardiac ejection fraction as determined by echocardiography.
Surgery
Aortic valve replacement is the only possible method of valve correction.
It is recommended for patients with:
- severe aortic regurgitation and the presence of symptoms regardless of ejection fraction;
- asymptomatic chronic severe aortic regurgitation and ejection fraction less than 50%;
- chronic aortic regurgitation in parallel with coronary artery bypass surgery or surgery on the aorta and other heart valves;
- asymptomatic severe aortic regurgitation with normal ejection fraction. on significant expansion of the left ventricle (EDV - more than 75 mm).
The duration of treatment for patients with aortic insufficiency varies greatly depending on the severity of the condition and the cause of the pathology. After the operation, it is recommended to undergo a course of rehabilitation in a cardiological sanatorium or rehabilitation center. The recovery period is at least 3 months, after which the patient can resume work with the doctor’s permission.
Complications
Complications of aortic insufficiency develop as its severity increases. At the beginning, normal syncope (fainting) may appear due to insufficient blood supply to the brain. Conduction disorders in the form of blocks of the left bundle branch and atrioventricular conduction of impulses can also often occur in patients with aortic insufficiency.
Coronary insufficiency can accompany aortic insufficiency, but more often in combination with aortic valve stenosis. The patient develops attacks of angina (pain in the heart of a pressing, squeezing nature) and even myocardial infarction.
Heart failure is the most common complication of already severe aortic regurgitation. The patient complains of shortness of breath during physical exertion, asthma attacks, and swelling of the lower extremities.
Sudden death often develops as a result of life-threatening arrhythmias - paroxysmal ventricular tachycardia, ventricular fibrillation. In this case, the person does not even have time to call an ambulance - the arrhythmia develops so quickly.
Classification of congenital heart disease
A doctor examining a patient whose aortic valve has only 2 instead of 3 leaflets is obliged and adheres to a certain classification of the disease. This is very important in terms of further tactics and treatment.
The classification criterion is the anatomical feature of the structure of the valve apparatus. During embryogenesis, the valves fuse and sutures appear between them. Whether the child will have a pathology or not depends on how correctly this process goes.
Normal and V types of 2-leaf aortic valve (I is the most common)
In patients with the described congenital heart defect, 3 main characteristics of the valves are examined - their size, the characteristics of the sutures between them, and the level of smoothness of their edges. The most common option is complete fusion of the right and left valves. The second most common pathology is the presence of a suture that is in unnatural positions.
To summarize, there are 3 types of configurations of bicuspid aortic valves (5 typical varieties are shown in the photo above):
- with two doors that are completely symmetrical to each other;
- with three valves, but two of them merge;
- with three leaves, but the three leaflets merge.
Its further development and symptoms depend on the anatomical features of the disease. That is why it is important for the doctor to determine a specific diagnosis.
Complications
It should also be noted that the disease has some complications, which must be indicated when making a diagnosis. The most common of them are calcification and/or stenosis of the aortic valve, dilatation of the aorta, reverse blood flow through the valve, and infection of its leaflets.
Normal and calcified aortic valve with 2 leaflets instead of 3
Calcification of the bicuspid aortic valve most often occurs in older people, and will produce a murmur in the clinic. When the valves cannot close completely, regurgitation or backflow of blood into the heart will occur.
Interesting fact. BAV is the most common heart defect occurring in people with the genomic disease Shereshevsky-Turner syndrome.
In addition, lesions of the aorta lead to its aneurysm, the rupture of which, in most cases, leads to death. And the last complication worth mentioning is narrowing of the aorta. It leads to a partial or complete cessation of blood flow from the heart.