Author: Strokina O.A., therapist, functional diagnostics doctor. February, 2021.
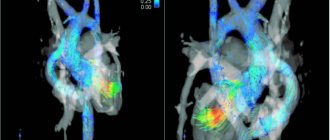
One of the most informative methods for studying the heart is scintigraphy (nuclear scanning). To carry out the procedure, a medication containing radioactive isotopes (radionuclides) is used. The drug is injected into the patient's body intravenously and, circulating in the bloodstream, is gradually absorbed by the heart muscle.
Based on the degree of saturation of myocardial tissue with radionuclides, experts evaluate its functionality: active absorption indicates normal heart function, and vice versa, “empty” areas may indicate ischemia (death) of cardiac tissue.
Perfusion scintigraphy is a specific method for diagnosing coronary heart disease (CHD) using radioactive thallium. The procedure is performed with functional tests, and unlike conventional electrocardiography (ECG) and even echocardiography (ultrasound of the heart) with physical activity, it allows you to most accurately determine the location of the ischemic zone.
How is coronary stenting different from open surgery?
Coronary stenting is a type of percutaneous coronary intervention (PCI). Unlike open-heart surgery, coronary stenting is characterized by a minimal degree of trauma to the patient: the stent is implanted through a small puncture in a vessel of the thigh or upper limbs. This type of surgery does not require the use of general anesthesia: the patient is conscious and watches what is happening on the angiograph screen. In addition, treatment using endovascular surgery techniques is quick and comfortable, and the patient goes home the very next day after stenting the heart vessels.
If the stent implantation is successful, the patient feels relief almost immediately. Since normal blood flow to the heart is restored, heart pain, shortness of breath and other unpleasant signs of IHD disappear. Coronary artery stenting normalizes blood flow by widening and opening up narrowed and blocked arteries. As a result, chest pain decreases or completely disappears; physical activity does not provoke painful conditions.
Successful surgery minimizes the need for coronary artery bypass graft surgery in the future, where a vein or artery is removed from a part of the body and sutured directly to the heart to avoid affecting the affected area. Such an intervention requires an incision in the chest, but the risks are greater and the recovery period is longer. In addition, the price of cardiac stenting is much lower than bypass surgery.
Myocardial scintigraphy results
When reading the scintigraphy results, the doctor can determine:
- intensity of coronary circulation;
- degree of blood supply insufficiency;
- localization of necrotic areas;
- foci of ischemia during exercise;
- scars after a heart attack.
Also, based on the results of the study, the likelihood of developing possible complications is calculated, a program of conservative treatment is planned, or the method of surgical intervention is determined.
Scintigraphy is not informative in assessing the size of the heart and the condition of the coronary vessels. That is, this method will not allow one to determine the location and degree of narrowing of blood vessels.
Indications
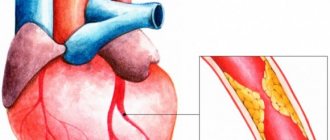
In what cases is stenting of coronary vessels performed? Often the reason for this is atherosclerosis. It begins due to the accumulation of cholesterol molecules on the walls of the arteries, gradually forming plaques. This complicates blood flow in this area, and the heart muscle experiences a lack of oxygen. As a result, the patient develops coronary disease, the symptom of which is angina pectoris. Retrosternal pain or pain in the heart area, shortness of breath, weakness, make themselves felt during physical activity. Read more about the characteristic signs of an angina attack here.
Cardiac stenting helps prevent the dangerous consequences of coronary artery disease: heart attack and acute coronary syndrome. Coronary stenting is a help for advanced stages of the disease or for emergency treatment of acute coronary syndrome. However, if both vessels are affected or the diameter of the vascular lumen is too small, bypass surgery, an open operation, will give better results.
Indications for cardiac scintigraphy
Doctors can recommend cardiac scintigraphy both to patients who have already identified certain heart pathologies, and to patients for whom it is impossible to make a diagnosis due to lack of information. After receiving the results, the doctor will plan further treatment tactics and determine the diagnosis. It is worth noting that this method can act as both primary and additional.
First of all, representatives of the risk group for developing IHD (coronary heart disease) should think about undergoing a heart scintigraphy procedure as a preventive measure:
- long-term heavy smokers;
- people with high cholesterol;
- patients with hypertension and/or diabetes;
- men over 45 years of age and women over 55 years of age.
This diagnosis is prescribed in situations where it is necessary to assess the effectiveness of the prescribed course of treatment as accurately as possible. In addition, the study is recommended for athletes before competitions and patients who are scheduled for surgery or other manipulations on the heart.
Scintigraphy is also prescribed to patients who have had a heart attack, because the technique allows you to assess the performance of the heart muscle. Angina pectoris is also an indication for scintigraphy.
Very often people complain of pain of unknown origin in the chest area. Most people do not pay attention to this, although this may be the first signal of the development of a dangerous heart disease. Doctors recommend that when the first such symptoms appear, immediately contact a specialist who will most likely give you a referral for heart scintigraphy, because this technique is the most informative and reliable. Today, scintigraphy in Moscow is done in almost every large medical center, so no one should have problems finding a suitable institution.
Possible complications:
Coronary stenting rarely causes complications, but there are certain risks associated with it:
- Repeated narrowing of blood vessels (stent restenosis). If angioplasty is performed without stent implantation, the probability of restenosis reaches 30-40%. Installation of a bare metal stent reduces the possibility of relapse to 20%, and drug-coated stents - to 1%.
- The occurrence of blood clots. After some time, blood clots can form inside the stents, which are dangerous because they lead to a heart attack. To reduce the likelihood of their occurrence to a minimum, we recommend taking antiplatelet medications prescribed by your doctor: Plavix, aspirin, etc.
- Bleeding from the catheter site (arm or leg). In most cases, there will only be a slight bruise, but there is still a risk of serious bleeding.
Rare complications:
- Myocardial infarction or heart attack.
- Coronary artery rupture or dissection. Damage requires coronary artery bypass grafting or emergency stent graft implantation.
- Impaired kidney function. The contrast agent administered during stenting and angioplasty has a detrimental effect on the kidneys. If the patient already has problems with their functioning, the doctor prescribes medications for protection.
- Stroke. During surgery, blood clots may form on the catheter. If they fragment, break off and travel to the brain, the patient will suffer a stroke. To reduce the risk of developing this complication, blood thinning medications are used.
- Arrhythmia. Manifested by heart rate disturbances: bradycardia or tachycardia. This is a temporary complication that goes away after the medication is administered. A temporary pacemaker is rarely required.
Diagnosis of cardiac diseases
If there are symptoms indicating cardiovascular disease, it is necessary to conduct a comprehensive instrumental and laboratory examination to confirm the diagnosis, study the extent of the spread of the disease and search for the causes of its occurrence. Cardiology uses a wide range of instrumental and laboratory diagnostics.
— Blood tests (complete blood count, biochemical blood test, hemostasis, serology, immunology, cardiac enzymes)
Changing a number of blood parameters helps assess the degree of heart performance. For example, elevated cholesterol levels (can be a sign of coronary heart disease), abnormal levels of thyroid hormones (can affect heart rhythm), cardiac enzymes (chemicals released from damaged heart muscle cells indicate a myocardial infarction).
— Determination of the level of specific cardiac enzymes in the blood
Blood samples taken over a number of days will help identify the dynamics of changes in the level of enzymes - specific blood proteins that increase against the background of a developed myocardial infarction and decrease with recovery.
— Chest X-ray
The study allows you to evaluate the size and shape of the heart; detect the presence of fluid in the lungs, which may be evidence of ineffective heart function.
— Angiography of the vessels of the neck and brain (cerebral angiography)
An invasive method for diagnosing the location and degree of narrowing of the lumen of the vessel(s), based on the introduction of an iodinated contrast agent into the vascular bed with simultaneous fluoroscopy (radiography) of the neck and brain in patients at high risk of stroke.
— Coronary angiography
Complex invasive diagnostic test. Used to determine indications for surgical intervention in patients diagnosed with coronary heart disease and angina pectoris. This is an x-ray diagnostic method based on studying the passage of a contrast agent through the coronary vessels with subsequent assessment of the degree of their damage (narrowing).
— Echocardiography
Ultrasound scanning allows you to visualize the work of the heart, evaluate the structure (size of the chambers, thickness and structure of the walls), the functional viability of the heart valves and the heart as a whole. A painless examination, especially necessary for patients who have had a myocardial infarction, have heart failure or patients with heart valve diseases.
- Functional diagnostics
Electrocardiogram (ECG)
Shows the nature of the “electrical activity” of the heart (the rhythm of the heart). Allows you to identify the thickness of the heart muscle (myocardial hypertrophy against the background of high blood pressure), determine the area of myocardial damage after a heart attack, assess the adequacy of blood flow to the heart muscle, etc.
Electrocardiography with physical activity (treadmill test)
Assessment of the state of the heart against the background of physical activity (adequacy of blood supply to the myocardium in conditions of “increased demand”). A good way to diagnose obstruction of the patency of the coronary arteries.
Holter monitoring
The test is also known as a 24-hour ECG. An ECG is recorded within 24 hours to diagnose possible heart rhythm disturbances
— Multislice computed tomography (MSCT)
Computed tomography of the heart or assessment of coronary calcification (CT calcium scoring)
MSCT (multislice computed tomography) of the coronary vessels ( CT coronary angiography, CT cardiac angiography )
CT angiography of cerebral vessels, aorta, large vessels
CT scan of the brain
— MRI
MRI of the heart
MRI of the brain
Vascular MRI
— Radioisotope study of the heart (single-photon emission computed tomography)
One of the most modern and promising diagnostic methods. It is based on the use of radioactive isotopes (thallium 201 and technetium 99 atoms) and recording their distribution in the cardiovascular system using gamma radiation detectors. Allows you to assess myocardial perfusion, visualize the passage of blood through the heart and great vessels, conduct a differential diagnosis of myocardial ischemia, determine the location and size of the infarction, assess the nature of metabolic disorders in the heart muscle (determine the degree of viability of myocardial cells).
Preparing for stenting
After reviewing your medical history and performing a physical examination, the surgeon performs a coronary angiogram to determine whether atherosclerosis can be treated with stenting. A coronary angiogram makes it clear whether the arteries are narrowed or occluded (completely blocked). A contrast agent is injected through a catheter (a thin long tube passed to the coronary vessels through the artery of the leg or arm. When the substance fills the lumens of the arteries, X-rays are turned on. The image is displayed on the monitor, and the doctor determines exactly where the coronary arteries are affected. Having scheduled heart surgery, The doctor will give recommendations regarding nutrition. It is usually recommended to avoid drinking water and food after dinner the night before stenting. If you are undergoing preparation in the hospital, the instructions may be different.
The evening before surgery you should:
- Take medications prescribed by your doctor. If you are taking diabetic or blood thinning medications, your surgeon may ask you to stop taking them that evening.
- Prepare the necessary medications that you will take with you to the hospital.
- You will stay in the hospital until the next morning. Driving is contraindicated, so you should arrange your delivery home in advance.
Progress of percutaneous coronary intervention:
1. The site of exposure is treated with an antiseptic. The patient is given a local anesthetic and blood thinning medications to prevent the formation of blood clots. Small electrodes are attached to the chest to help the surgeon monitor the heart rhythm and pulse rate. 2. The operation is performed through the femoral artery (on the leg) or the radial artery (on the arm). Through a small puncture, a catheter-port for carrying instruments (introducer) is installed. Through it, a catheter is delivered to the mouth of the coronary artery, with the help of which surgical intervention is performed. 3. Angioplasty of the coronary arteries with stenting is performed in an angiographic operating room equipped with high-tech medical equipment. Contrast liquid is injected through the installed catheter. Using a coronary angiogram, the doctor evaluates the affected area. 4. A balloon catheter is passed to the site of the lesion, expanding the narrowed area. As the balloon inflates, the patient may feel discomfort in the chest. This is due to the blocking of blood flow through the artery - after the balloon is deflated, the unpleasant sensation stops. Stent implantation: 1. The stent, mounted in a closed state on a balloon, is advanced to the narrowed area of the artery. 2. The surgeon inflates the balloon in the affected area, thereby expanding the stent. 3. The wire remains in the artery to keep it open and improve blood flow to the heart. 4. The surgeon removes the catheter and makes control coronary angiograms to assess the strength of blood flow through the dilated artery. 5. The doctor applies a pressure bandage to the area of the leg or arm where the catheter was inserted.
Coronary stenting takes from 30 minutes to several hours, depending on the severity of atherosclerosis. As prescribed by your doctor, after surgery you should take medications that minimize the possibility of blood clots. For a video of stenting of cardiac vessels, follow the link.
Rehabilitation
The patient spends the first few hours in the intensive care unit, where the doctor monitors blood pressure levels and heart parameters. If there are no contraindications, during rehabilitation it is recommended to drink more fluid (about two liters per day) so that the body quickly removes the contrast fluid. It is better to avoid heavy lifting and intense exercise. A few days after discharge from the hospital, the patient returns to his normal life.
After surgery, it is important to strictly follow the doctor’s recommendations and attend scheduled cardiologist appointments on time. Taking blood-thinning drugs: aspirin (Cardiomagnyl, thrombo ACC, Cardiasca, etc.) and clopidogrel (Plavix) requires special attention.
Myocardial scintigraphy (myocardial perfusion scintigraphy) is a study of the blood supply (perfusion) of the left ventricular myocardium using radiopharmaceuticals (RPs), which are distributed in healthy heart tissue. The radiopharmaceutical is administered intravenously and accumulates in the heart muscle, then the radiation from the accumulated drug is captured by the detectors of the recording device.
Myocardial scintigraphy is a unique diagnostic method that makes it possible to objectively assess the blood supply to the heart muscle.
Indications for myocardial perfusion scintigraphy:
- Detection and differential diagnosis of coronary heart disease (CHD): Angina pectoris and stable angina pectoris, episodes of unstable angina pectoris.
- Assessment of the significance of coronary artery lesions in patients diagnosed with coronary artery disease.
- Assessment of the risk of cardiovascular complications (myocardial scintigraphy is performed if the diagnosis of coronary artery disease has already been made).
- Evaluation of the effectiveness of coronary angioplasty, bypass surgery and thrombolysis; assessment of the effectiveness of revascularization.
- Repeated scintigraphy for resumption of angina after interventions on the coronary vessels.
- Confirmation of the diagnosis of acute myocardial infarction (AMI) in the presence of a questionable ECG.
- Study of the blood supply to the myocardium of the left ventricle in its non-coronary lesions (cardiomyopathies, myocarditis, early complications of diabetes mellitus).
- Determination of treatment strategy and quality control of treatment provided.
There are 2 options for performing myocardial perfusion scintigraphy:
- Myocardial scintigraphy at rest - performed within 1 day.
- Myocardial scintigraphy at rest and with load (bicycle ergometry) - carried out over 2 days.
According to experts, scintigraphy of the myocardium at rest, i.e. without stress test, not very informative.
However, in some cases this diagnostic method is indicated for:
- Chest pain of unknown etiology.
- If it is impossible to perform physical activity, permanent cardiac pacing (PAC), left bundle branch block (LBBB).
- Asymptomatic disorders during other stress tests and when they are not informative.
Due to the current impossibility of performing a functional load, myocardial perfusion scintigraphy is performed only at rest.
When studying cardiac perfusion at rest, it is actually possible to confirm the presence of scar changes (infarct zones) of the myocardium, as well as assess blood supply, while studying the myocardium at rest and with stress expands the diagnostic capabilities of the technique.
Contraindications for scintigraphy:
- pregnancy, restriction during breastfeeding (cancellation for 48 hours).
to perform a load test:
- myocardial infarction in the last two days (48 hours);
- unstable angina with a high risk of cardiovascular complications;
- untreatable arrhythmias accompanied by hemodynamic disturbances;
- severe clinical aortic stenosis;
- severe heart failure;
- pulmonary embolism;
- dissecting aortic aneurysm;
- acute myocarditis, pericarditis or infective endocarditis;
- severe non-cardiac diseases that may affect the performance of the test, or may worsen during the test (including infections, renal failure, thyrotoxicosis);
- severe emotional disorders, psychoses.
Preparing for the study
If you plan to do only the study at rest, medications are not canceled.
During exercise tests, after consultation with your doctor, it is recommended to discontinue β-blockers (atenolol, bisoprolol, nebivolol, etc.) 3 days before the exercise test.
Features of the study: it is advisable to conduct a stress test of the heart as part of hospitalization in a hospital for several days to monitor the patient’s condition before and after the stress test and conduct additional diagnostic tests.
The study is carried out strictly on an empty stomach, and have full-fat yogurt (sour cream or cheese) with you.
The procedure is carried out 30–60 minutes after the administration of the radiopharmaceutical and takes up to 30 minutes.
The conclusion is issued on the day of the study.
Patients must have with them an extract from the outpatient card/medical history with an examination by a cardiologist or therapist, an archive of electrocardiograms, the results of heart studies, if available (ECHOCG, Holter monitor, ABPM, VEM, Treadmill test, etc.), which he must provide to the radiologist.
To examine the patient under load, you must bring comfortable shoes and sweatpants for bicycle ergometry.
Cost of radioisotope research:
| Service code | Name of service | Cost, rub. |
| A07.03.001.001 | Whole body bone scintigraphy | 8 700 |
| A07.03.001.002 | Whole body bone scintigraphy combined with single photon emission computed tomography of bones and computed tomography of the thoracic spine | 20 500 |
| А07.03.001.003 | Whole body bone scintigraphy combined with single photon emission computed tomography of bones and computed tomography of the lumbosacral spine | 27 500 |
| A07.03.001.004 | Whole body bone scintigraphy combined with single photon emission computed tomography of bones and computed tomography of the pelvic bones | 27 500 |
| A07.03.003 | Single photon emission computed tomography of bones | 7 400 |
| A07.09.004 | Single photon emission computed tomography of the lungs (perfusion) | 14 000 |
| A07.09.004.001 | Single-photon emission computed tomography of the lungs (perfusion), combined with computed tomographic angiography of the pulmonary artery and its branches | 29 300 |
| A07.10.003 | Single-photon emission computed tomography of the myocardium at rest | 8 800 |
| A07.10.003.002 | Single-photon emission computed tomography of the myocardium, perfusion with functional tests | 15 700 |
| A07.10.005 | Single photon emission computed tomography combined with myocardial computed tomography | 18 800 |
| A07.14.002 | Scintigraphy of the liver and spleen | 9 800 |
| A07.14.002.002 | Liver scintigraphy with labeled red blood cells | 22 200 |
| A07.14.004.001 | Single-photon emission computed tomography of the liver and spleen combined with computed tomography of the hepatobiliary zone | 19 800 |
| A07.22.002 | Thyroid scintigraphy | 6 500 |
| A07.22.010 | Single photon emission computed tomography of the parathyroid glands | 9 600 |
| A07.22.010.001 | Single photon emission computed tomography of the parathyroid glands combined with computed tomography of the parathyroid glands | 29 700 |
| А07.28.002 | Scintigraphy of the kidneys and urinary system | 8 700 |
| A07.28.004 | Angionephroscintigraphy | 8 000 |
| A07.30.031 | Three-phase scintigraphy of soft tissues and bones | 11 400 |