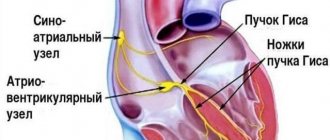
Home / Encyclopedia of diseases / Diseases on A / Aortic aneurysm
Aortic aneurysm is an enlargement of a section of the aorta caused by a pathological change in the connective tissue structures of its walls due to an atherosclerotic process, inflammatory lesion, congenital defect or mechanical damage.
Depending on the location of the aneurysm, aneurysms of the thoracic aorta, thoraco-abdominal (thoracic-abdominal) aorta and abdominal aorta are distinguished. In turn, thoracic aortic aneurysm can be divided into aortic sinus aneurysm, ascending aortic aneurysm, aortic arch aneurysm and descending aortic aneurysm.
In addition, a special category is a dissecting aortic aneurysm - a pathological cavity or canal formed in the thickness of the aortic wall as a result of its dissection with blood pumped from the lumen of the aorta through a defect in the intima (inner lining of the vessel) resulting from a pathological process or damage. Dissection of the aortic wall occurs inside its tunica media.
Symptoms of aortic aneurysm
Aortic sinus aneurysm may be accompanied by aortic valve insufficiency or narrowing of the lumen of the coronary arteries of the heart. Reaching a large size, such an aneurysm can compress the pulmonary trunk, right ventricle and right atrium, which leads to the formation of subacute right ventricular heart failure, characterized by liver enlargement, swelling of the jugular veins and the appearance of edema. Rapid compression of the pulmonary trunk by an aneurysm can lead to sudden death of the patient.
An aneurysm of the ascending aorta is usually manifested by dull retrosternal pain, which in some patients is accompanied by reflex attacks of shortness of breath. If the aneurysm reaches a large size, it can cause atrophy of the adjacent areas of the sternum and ribs, with pathological vascular pulsation appearing in the second or third intercostal space to the right of the sternum. Compression of the superior vena cava by an aneurysm or a breakthrough of the aneurysm into it leads to the development of superior vena cava syndrome, which in turn causes swelling of the neck, face, arms, and swelling of the jugular veins.
Aneurysm of the aortic arch most often manifests itself as shortness of breath (and, as a rule, it is more difficult to take a breath), caused by compression of the trachea and bronchi. Compression of the left main bronchus by an aneurysm can lead to atelectasis (collapse) of the left lung. Sometimes hemoptysis appears, which may precede the rupture of an aneurysm. Compression of the left inferior laryngeal nerve by an aneurysm is manifested by a dry cough, attacks of suffocation, and a change in voice timbre (hoarseness). The development of superior vena cava syndrome is possible. When an aneurysm compresses the brachiocephalic trunk, left subclavian and left common carotid arteries, symptoms of a gradually worsening disturbance of the blood supply to the upper extremities and head appear. A rupture of an aortic aneurysm into the esophagus or trachea is possible, which, as a rule, develops gradually, which is initially manifested by the appearance of scanty bloody vomiting or hemoptysis, but then massive bleeding develops.
An aneurysm of the descending aorta leads to compression of the nerve roots, vertebral bodies, esophagus and left lung. Compression of the nerve roots leads to intense pain that is resistant to the administration of the most powerful painkillers. Pressure on the vertebral bodies and posterior parts of the ribs leads to their deformation, to the point that the aneurysmal sac can protrude between the inner edge of the left scapula and the spinal column. These patients may develop lower paraplegia (complete loss of voluntary movements of both lower extremities). Compression of the left lung by an aneurysm leads to its atelectasis and creates favorable conditions for the occurrence of pneumonia. Compression of the esophagus in some cases can lead to difficulty passing food through it (dysphagia). When the wall of the esophagus is destroyed due to prolonged pressure on it from the aneurysm, small bleeding from the esophagus occurs, after which, as a rule, the aneurysm ruptures into its lumen with the development of massive bleeding. When a descending aortic aneurysm ruptures into the pleural cavity, rapidly increasing anemia (anemia) and large hemothorax (accumulation of blood in the pleural cavity) develop.
Aneurysm of the thoracoabdominal (thoracoabdominal aorta) aorta is rare and is usually caused by syphilis. The aneurysm compresses the esophagus and upper stomach, which leads to pressing pain in the epigastric region, which can be associated with food intake, sometimes belching, vomiting, and disruption of the passage of food through the esophagus. An aneurysm of the thoracoabdominal aorta can cause narrowing or complete occlusion of the lumen of the superior mesenteric artery and the celiac trunk, which supply blood to the abdominal organs, which is manifested by attacks of painful abdominal pain (the so-called abdominal pain). Due to the reasons described above, an aneurysm of this location leads to weight loss for the patient.
An abdominal aortic aneurysm over time manifests itself as pain caused by the pressure of the aneurysm on the nerve plexuses and nerve roots located directly next to it. Pain may be in the lumbar or epigastric region. A large aneurysm located below the origin of the renal arteries can compress the ureters, causing the development of hydronephrosis and anuria. If compression of the renal arteries occurs, symptomatic hypertension occurs. When the duodenum is compressed by an aneurysm, the passage of food through it is disrupted, which is manifested by vomiting and weight loss. Most often, an abdominal aortic aneurysm is manifested by the presence of a pulsating tumor-like formation in the abdominal cavity at the level of the navel or just below and slightly to the left of it. A thrombosed aneurysm does not pulsate, and therefore can be mistaken for a tumor. Sometimes there is a rise in body temperature. An aneurysm ruptures into the abdominal cavity quickly and, as a rule, painlessly, and into the retroperitoneal tissue - with severe pain in the abdomen and lower back, with the development of shock. After some time, the patient may die due to increasing blood loss.
Dissecting aortic aneurysm is manifested by sudden onset of acute chest pain that is not relieved by painkillers and collapse. Sometimes a complete loss of the ability to voluntarily move both lower extremities develops, which can be temporary or permanent. Due to the localization and nature of the pain that occurs, the clinical manifestations of dissecting aortic aneurysm can be mistaken for acute myocardial infarction.
WHEN TO CONTACT THE DOCTOR
When the above symptoms appear.
You can make an appointment with a cardiologist at Medical by calling 8 (49244) 9-32-49.
Symptoms of the disease
As a rule, the disease occurs without symptoms. In most cases, an aneurysm is discovered accidentally - during a routine examination. If symptoms appear, they are expressed in the area of the aortic arch. Some of the most striking signs of the development of the disease include:
- heavy snoring;
- shortness of breath, cough;
- sharp chest pain;
- discomfort during swallowing.
In some cases, individual signs of a cardiac aortic aneurysm may appear.
Diagnosis of the disease
Diagnosis of the disease begins with the patient visiting a therapist. In this case, the specialist collects anamnesis, analyzes the existing symptoms, and then refers the patient to a highly specialized specialist. To confirm the diagnosis, additional laboratory and hardware tests are prescribed:
- clinical, general urine and blood tests: allow you to determine the presence of pathologies that affect the further development of the disease;
- echocardiography: helps determine the type, shape, size of the aneurysm;
- X-ray: shows enlarged heart, pulmonary edema.
In some cases, MRI of the heart vessels is prescribed to obtain important data.
Make an appointment Make an appointment and get a high-quality examination of the heart and blood vessels in our center
Prevention
When diagnosing this disease, it is important to resort to effective preventive measures. These include the following activities:
- maintaining a healthy lifestyle;
- refusal to drink alcohol, smoke;
- timely examination by a doctor.
In addition, the patient must form the correct diet. Meals for aortic aneurysm should be nutritious. At the same time, the menu should not include fatty foods. Sufficient physical activity is another component of prevention. If a patient has acute chest pain for more than 6 minutes, the patient should seek immediate medical attention.
Causes of aortic aneurysm
Most often, an aortic aneurysm develops as a result of an atherosclerotic process or is of syphilitic origin. Recently, atherosclerosis has taken first place among the causes of aortic aneurysm development, which is due to advances in the treatment of syphilis and an increase in average life expectancy. In addition, syphilis is more often the cause of the development of a thoracic aortic aneurysm, while atherosclerosis more often leads to the formation of an abdominal aneurysm.
Other causes of aortic aneurysm development are medianecrosis and nonspecific aortoarteritis. Traumatic aneurysms are also possible (for example, after a closed abdominal injury) and false anastomotic aneurysms after operations on the aorta. Aneurysms of mycotic (fungal) origin are also described in the scientific medical literature.
The most common cause of the development of dissecting aortic aneurysm is long-standing arterial hypertension against the background of atherosclerosis. In this case, on the inner lining (intima) of the aortic wall, as a rule, there are already various pre-existing small defects. Less commonly, the causes of dissecting aortic aneurysm can be hypertension due to coarctation of the aorta (a congenital defect manifested by segmental narrowing of the aortic lumen); arterial hypertension caused by other factors; Marfan syndrome (hereditary pathology of connective tissue), which is accompanied by severe weakness of the aortic wall. It is possible to form an acute dissecting aneurysm of the ascending aorta due to its rupture caused by a closed injury (for example, a car injury). Sometimes dissecting aortic aneurysm can occur as a result of iatrogenicity: as a complication of cannulation of the arteries and aorta for the purpose of perfusion during cardiopulmonary bypass.
Complications of aortic aneurysm
1. Aortic valve defects and heart failure . With an aneurysm of the ascending aorta of syphilitic origin, cardiac decompensation may develop due to a defect of the aortic valve or blockage of the mouth of the coronary arteries.
2. Rupture of an aneurysm with bleeding . Bleeding can occur into the respiratory organs (bronchi, trachea), pleural cavity, cardiac sac, into the esophagus, large blood vessels located in the chest cavity, and sometimes even out through the skin when the sternum is destroyed. In case of bleeding into the pericardial cavity, cardiac tamponade occurs. Bleeding results in rapidly increasing blood loss.
3. Acute and subacute thrombosis of the aortic aneurysm. Most often it develops in the abdominal aorta and leads to the closure of its branches located here.
The listed complications quickly lead to the death of the patient if appropriate measures are not taken in time.
Instrumental examination
X-ray examination. For aneurysms of the thoracic aorta, radiography is performed in three projections with mandatory contrasting of the lumen of the esophagus. The expansion of the shadow of the vascular bundle is characteristic. Aneurysms of the descending aorta bulge into the left pulmonary field. Most patients experience displacement of the contrast-enhanced esophagus. Sometimes calcification (calcification) of the aneurysmal sac is determined. In case of aneurysms of the abdominal aorta, plain radiography of the abdominal cavity in two projections allows us to identify calcification of the aortic wall and urination of the lumbar vertebral bodies.
Ultrasound examination (ultrasound) of the aorta and heart. Ultrasound allows us to identify the presence and size in diameter and along the length of aneurysms of the ascending, descending aorta, aortic arch, abdominal aorta, the condition of the vessels extending from the aorta, as well as the presence of aortic valve defect, the nature of changes in the aortic wall.
Computed tomography (CT). When the lumen of the aorta is more than 4 cm, its expansion is considered to be aneurysmal. When performing computed tomography, it is possible to determine the involvement of large arteries in the process and identify signs of dissection (dissection) of the walls (in case of dissecting aortic aneurysm). Angiographic examination (aortography). It is used, as a rule, before surgery when planning its nature and volume.
Material and methods
The study was conducted on 123 hearts taken at autopsy in city pathological and forensic departments from the corpses of patients of both sexes aged from 28 to 87 years (35 men and 57 women) who died from causes not related to diseases and injuries of the heart. The hearts were removed as a single complex along with the lungs, mediastinum, diaphragm and organs of the upper abdominal cavity. The heart chambers were washed with warm water to remove blood clots and blood clots. Through a cannula inserted into the thoracic aorta, after ligation of the large vessels of the aortic arch and coronary arteries, a solution of warm water was injected under a constant hydrostatic pressure of 0.18 bar, equivalent to 140 mmHg. to determine AA deficiency. In cases where the pressure in the aorta dropped rapidly, such hearts were assigned to the group with aortic valve insufficiency (group 2), which consisted of 15 hearts. The remaining hearts were assigned to the control group with preserved valve closure function (group 1), amounting to 108 hearts. Fixation of the preparations was carried out by continuous perfusion of an 8% formalin solution injected through a cannula into the aorta under a pressure of 0.18 bar (140 mm Hg) and into the superior vena cava under a pressure of 0.02 bar (15 mm Hg). within 5 days.
For the study, morphometric methods were used on freshly fixed preparations, on preparations made by silicone plastination at room temperature, as well as on preparations of hearts in which the chambers and large vessels were filled with a polymerized colored silicone composition with the addition of radiopaque red lead. In addition to morphometry, injected and plastinated hearts were examined using computed tomography and magnetic resonance imaging.
To prepare an injectable colored radiopaque silicone composition, a mixture of 92 parts by mass of SKTN E grade silicone, 5 parts by mass of red lead and 3 parts by mass of hardener K-1 was used. All components were thoroughly mixed until a homogeneous mass was obtained immediately before injection. A radiopaque composition was injected through a cannula installed into the ascending aorta at a pressure of 100 mmHg. Art., which contributed to the closure of A.K. The left ventricle and left atrium were filled through a cannula inserted into the left atrial appendage at a pressure of 20 mm Hg, which allowed filling the left chambers of the heart and maintaining their natural shape. To accelerate the polymerization of silicone, the organocomplex of the heart and lungs was immersed in warm water for 3-4 hours. This injection technique made it possible to maintain the relationship between the original geometry of the aortic root and the intracardiac structures of the left parts of the heart with the A.C. closed. After the silicone hardened, computed tomography of the injected heart was performed, after which modified preparation and morphometry techniques were used.
In all preparations, the circumference of the cross section of the ascending aorta, sinotubular junction (SJ), basal ring of the aorta, the length of the base and height of the intercuspid triangle of the aorta were measured (Fig. 1).
Rice. 1. Photograph of the parameters of the interleaf triangle by A.K. The aorta and left chambers are injected with silicone. 1 — length of the base of the inter-flap triangle; 2 — height of the inter-flap triangle. as well as the magnitude of the deflection angle of the inter-flap triangle (Fig. 2).
Rice. 2. Three-dimensional reconstruction of the AC on a multislice computed tomogram. The angle of deviation (α) of the inter-valvular triangle of the AC from the plane of the longitudinal section of the ascending aorta. The area of the intervessel triangle and AC regurgitation were also calculated using the formulas:
S
tr.=
p
(
p
–
a
)(
p
–
b
)(
p
–
c
),
S
reg.=π·
r
2,
where S
tr.
- area of a triangle; a
,
b
,
c
- sides of the triangle;
p
is the semi-perimeter of the triangle;
where S
reg.
- area of regurgitation; r
is the radius of regurgitation.
Measurement of the angle of deviation of the inter-valvular triangles of the AC from the plane of the longitudinal section of the aortic root was carried out using multislice computed tomography (MSCT) preparations (see Fig. 2). The base of the inter-valvular triangle is a straight line drawn from the lower point of attachment of one semilunar valve to the aortic wall to the lower point of attachment of the other. The apex of the inter-flap triangle is the upper point of the commissure of the AK flap.
After the measurements, the AC valves were assessed for the presence of commissural fenestrations. Particular attention was paid to the areas of the valves at the site of their attachment to the aortic wall and to the apex of the inter-valve triangle. Morphological changes were assessed according to the degree of degenerative changes: degree I - the presence of changes only in the semilunar valves (thinning, discoloration, atherosclerotic changes) without their calcification; II degree - the presence of changes in the semilunar valves (thinning, discoloration, atherosclerotic changes) in combination with fenestrations in the commissural areas of the valves and/or the presence of calcification of the aortic wall; III degree - the presence of changes in the semilunar valves (thinning, discoloration, atherosclerotic changes) in combination with fenestrations in the commissural areas of the valves and the presence of calcification in the inter-valve triangles.
Statistical processing of the obtained data was carried out using the IBM SPSS (Statistical Package for the Social Sciences) program version 20.0 for Windows. The method of multiple logistic regression analysis was used. The level of statistical significance of the differences was taken as 0.05.
Treatment of a patient with an aortic aneurysm
A thoracic aortic aneurysm with a diameter of more than 5 cm is subject to surgical treatment due to the high risk of its rupture and the development of thromboembolic complications. The surgical intervention is performed under conditions of artificial circulation and hypothermia (low temperature) and is reduced to resection (removal) of the aneurysm with simultaneous replacement of the removed area with a prosthesis.
In case of an asymptomatic course of an abdominal aortic aneurysm, the indication for planned surgical intervention is its diameter of more than 4 cm. In cases of increasing pain and the threat of rupture, emergency surgical intervention is indicated. The operation is reduced to resection of the aneurysm with direct replacement of the abdominal aorta or bifurcation aortofemoral replacement.
Diagnostics
Due to the absence of clear symptoms and gradual expansion of the aorta, most often the suspicion of an aneurysm appears to the doctor during an examination for another reason. The diagnosis is confirmed using ultrasound or CT scan of the abdominal cavity, angiography - which examination is suitable for a particular patient is decided by the attending physician. Examinations will provide information about the size of the aneurysm, the presence of a blood clot in this location, and the condition of the vessel walls.
In many patients, the identified dilatation of the aorta does not require surgical intervention by a specialist for a long time - the main task will be observation. In this case, the patient will be given a list of recommendations so as not to worsen the condition of the blood vessels (first of all, quitting smoking, if such an addiction is present), and will also be offered to undergo periodic examinations to monitor the condition of the aorta. But in any case, the doctor must exclude the risk of aortic rupture at the site of expansion. For this purpose, examination data is used: the width of the aorta and the rate of its expansion over time. If there is a threat of rupture, the doctor may decide to perform an operation, and this will require additional tests of blood, blood vessels, and urine to prepare for the operation.
Prognosis for aortic aneurysm
In the absence of timely treatment and the occurrence of severe complications of aortic aneurysm, the prognosis is unfavorable. Death can occur as a result of decompensation of cardiac activity caused by the development of aortic valve defects with an aneurysm of the ascending aorta, cardiac tamponade due to the breakthrough of an aneurysm into the pericardial cavity, massive blood loss as a result of a breakthrough of the aneurysm into the hollow organs and the pleural or abdominal cavity.
However, the successes currently achieved in the surgical treatment of aortic aneurysms make it possible, in the case of timely and adequate surgical intervention, to save the lives of the majority of patients. With a planned operation, the mortality rate is 0-5%, and in the case of aneurysm rupture, even with emergency surgery, it is 50-80%. The five-year survival rate among operated patients is 80%, and among non-operated patients it is 5-10%.