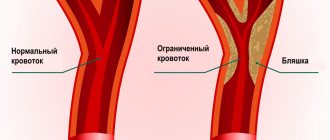
Atherosclerosis of the subclavian artery develops most often in the initial part of this artery and may be accompanied by the development of symptoms of circulatory disorders in the arm or cerebral circulatory failure due to the phenomenon of spinal-subclavian steal.
Treatment for blockage (occlusion) of the subclavian artery is only surgical, but both open and endovascular approaches are possible. The need for treatment is determined by the development of chronic circulatory failure in the arm and signs of cerebrovascular accidents.
Surgeons at our center have extensive experience in successfully treating patients with damage to the subclavian arteries. In most cases, these were endovascular stenting operations of the subclavian artery. In our clinic, it is possible to choose the optimal treatment method, since we have the capabilities of both open and endovascular interventions. In recent years, the endovascular method - angioplasty and stenting of the subclavian artery - has become the method of choice in our center, as it is safer for patients and gives good immediate and long-term results.
Causes and risk factors
The reasons for the development of atherosclerosis of the subclavian artery are the same as for other atherosclerotic plaques. Most often these are high cholesterol, diabetes, obesity, and smoking. Lesions most often occur in the initial section (proximally) of the subclavian artery, but can also occur in other segments. Damage to the subclavian artery may be associated with compression between the first rib and the clavicle (compression syndrome at the thoracic outlet). Proximal lesions of the subclavian artery can be insidious and are detected by measuring blood pressure on different arms or pulsations. However, complications related to blood circulation in the arm or brain often develop.
Course of the disease
Atherosclerotic occlusion gradually leads to worsening symptoms of chronic arterial insufficiency of the arm. Gradual muscle atrophy occurs, and cerebrovascular accidents may develop.
In general, subclavian artery occlusion poses little threat to life expectancy, but has a serious impact on quality of life, so treatment is indicated when symptoms are present.
The disease can be divided into several stages:
I (compensation). Occasionally, the patient complains of increased sensitivity to cold, a feeling of numbness, and weakness during physical activity.
II (partial compensation). "Intermittent claudication of the arm." It is characterized by symptoms of blood flow insufficiency - weakness, pain, numbness, coldness in the fingers, hand, and forearm muscles during physical activity. Transient disturbances of cerebral circulation are possible.
III – (decompensation). Permanent arterial insufficiency of the arm. The patient complains of constant numbness of the arm, a decrease in the volume of the shoulder and forearm compared to the other side, a decrease in muscle strength, and the inability to perform fine movements with the fingers.
IV – (trophic ulcers and gangrene). There appears cyanosis of the hand, swelling of the phalanges, cracks, trophic ulcers, necrosis and gangrene of the fingers.
Fortunately, such extreme manifestations are quite rare.
Vertebral artery syndrome with neck osteochondrosis
According to statistics, the majority of disorders (more than 70%) are degenerative-dystrophic changes in the body or osteochondrosis. The rest consists of congenital anomalies of the structure of the vertebrae or vertebral arteries, postpartum injuries, scars, tumors, herniated intervertebral discs and overgrown osteophytes, vertebral instability, etc.
Vertebral artery syndrome is a symptom complex of cerebral, vascular, and autonomic abnormalities that occurs as a result of compression of the vertebral arteries, deformation of their walls, or narrowing of the lumen of the blood canal.
Anatomy
The vertebral artery is a paired formation that arises from the subclavian arteries and runs in the canal formed by the openings of the transverse processes of the cervical vertebrae. After passing through the atlas and occipital foramen of the skull, the vertebral arteries merge into a single basilar artery, which supplies blood to the posterior parts of the brain. Any circulatory disorders immediately affect the nutrition of brain and nerve cells, causing severe headaches and dysfunction of the organs of vision and hearing.
On the one hand, the cervical spine has a rather delicate structure, a thin muscular corset and ligamentous apparatus, and does not have such reliable protection as other segments. On the other hand, he constantly experiences colossal loads (supports a fairly heavy skull, turns and tilts his head, etc.). Due to the natural deflection, the neck does not rest even during sleep.
In a normal healthy state under normal physiological conditions, the vertebral arteries are also compressed, limiting blood flow, but it is practically not impaired due to sufficient compensating conditions. The condition of the vessels can change due to anatomical narrowing of the lumen of the channels, atherosclerotic stenosis. Soft tissues, for example, the scalene or oblique muscles of the neck, can also have a compressive effect on the arteries, which intensifies after sharp turns or tilts of the head.
Degenerative-dystrophic changes in the body lead to disruption of metabolic processes in the cartilage of the intervertebral discs. Over time, the disc shell dries out, cracks, and flattens, pinching the vertebral arteries. Constant mechanical compression of blood channels entails chronic irritation of periarterial nerve clusters and the development of angiospastic syndrome (constant vasospasm).
Signs of vertebral artery syndrome
Functional symptoms of compression of the vertebral arteries:
- Headaches in combination with autonomic abnormalities. There may be pulsating, burning, aching, constant. As a rule, they originate in the back of the head, then spread to the temples, parietal and frontal parts. They intensify paroxysmally, especially during physical exertion (sudden movements of the head, after a long stay in a forced position, fast walking, running, with strong shaking in transport).
- Cochleovestibular disorders, manifested in the form of paroxysmal systemic or non-systemic dizziness. It manifests itself as a feeling of instability of the soil, rotation of surrounding objects or the body in space, instability of gait, and inability to maintain balance. Sometimes accompanied by slight hearing loss, inability to perceive a certain frequency of sounds.
- Visual disturbances are expressed in the flickering of butterflies or diverging circles before the eyes, pain, a feeling of sand, flashes. During an attack of severe headache, photophobia is noted. An ophthalmological examination shows a slight change in the tone of the vascular system of the fundus.
Organic symptoms accompanied by persistent impairment of cerebral circulation manifest themselves in the form of sudden dizziness, nausea, vomiting, difficult or slow articulation (the ability to pronounce sounds). Drop attacks (sudden falls with preservation of consciousness) lasting up to several minutes, loss of consciousness lasting up to 10 minutes may occur.
The attack usually subsides after the patient assumes a horizontal position. After the attack, there is a feeling of general weakness, sweating, tinnitus, irritation from bright lights, increased heart rate, blood pressure may increase, etc.
Neurological disorders include neuralgia of the occipital nerves, inflammation of the cervicobrachial plexuses, loss of sensitivity or reflex reactions of the lower part of the head, neck, shoulder girdle, and upper extremities. Torticollis may form - a forced tilt of the head, usually in the direction where the artery is pinched, and pain develops. The development of the disease against the background of existing cardiovascular pathologies is dangerous due to the occurrence of angina pectoris, coronary artery disease, etc.
Diagnosis and treatment
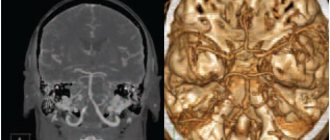
Diagnosing vertebral artery syndrome is quite difficult due to the variety of clinical complaints and symptoms. X-ray images do not always give a clear picture (changes are noticeable only in the bone structures of the spine), so an additional CT or MRI examination is required to identify the location and degree of vascular compression.
Magnetic resonance imaging can visualize in more detail intervertebral discs damaged by osteochondrosis, the presence of protrusions or hernias, subluxations of articular processes, vertebral hypermobility and other pathologies.
It is possible to identify compression of the vertebral arteries, their congenital anomalies of structure, and determine the asymmetry of the linear velocity of blood flow and the intensity of blood circulation in them using duplex scanning or vertebral Dopplerography. Tests are carried out both in a calm state (relaxed) and with functional loads (with flexion and extension of the neck, lateral bending, rotation).
From hardware diagnostics, electrocardiography and electromyography (determining the passage of nerve impulses) are mandatory. If necessary, a consultation with a cardiologist and neurologist is carried out.
Treatment of patients with vertebral artery syndrome requires an integrated approach. At first, it consists of complete rest, elimination of the compressive effect on blood vessels, reduction of neurogenic inflammation and traditional drug therapy:
- To relieve pain and inflammation - analgesics and non-steroidal anti-inflammatory drugs. In this case, anti-inflammatory drugs are best taken in the form of intravenous injections. Then they have a more gentle effect on the gastrointestinal tract, are more effective and the speed of onset of relief is much higher.
- Muscle relaxants are substances that relieve muscle spasms (relax muscles).
- Vasoactive drugs are prescribed to eliminate vascular inflammation and changes in the arterial bed, as well as to expand the lumen of the canals.
- Vitamins (a high content of B vitamins is especially useful) and anabolic agents - to activate trophic processes and improve the general condition of the body.
- Antidepressants and tranquilizers - for the correction of psycho-vegetative pathologies, improving emotional and psychological mood.
As the pain syndrome subsides, physiotherapeutic procedures (UHF, electrophoresis, ultrasound, etc.), massages, reflexology, and exercise therapy are added to the treatment.
If necessary, wearing a support collar (for example, Shants) and posture correction using traction (spinal traction) may be prescribed. The use of manual techniques (acupuncture, plantar and Thai massages, acupuncture, etc.), swimming, classical and passive yoga has a good effect. Author: K.M.N., Academician of the Russian Academy of Medical Sciences M.A. Bobyr
Complications
The most common complication is the phenomenon of vertebral-subclavian steal (steal syndrome). To compensate for blood circulation in the arm, cerebral blood flow is used, which moves in the opposite direction from the brain to the arm through the vertebral artery. In this case, physical work with the hand can cause disruption of cerebral circulation, including loss of consciousness.
Occasionally, atheroembolic complications may occur. Pieces of atherosclerotic plaque may be carried downstream into the arm. This is manifested by a sharp deterioration in blood circulation in the hand, blueness and pain in the fingers. If help is not given in a timely manner, necrosis of the finger may develop, which will require its amputation.
Forecast
Without treatment, atherosclerotic occlusion of the subclavian artery leads to a gradual decrease in working capacity, and the likelihood of ischemic stroke and gangrene of the hand increases.
After restoring blood circulation by any method, the problem is completely eliminated. Normal blood flow promotes normal hand function and eliminates brain steal syndrome.
Relapses after stenting of the subclavian artery occur in approximately 10% of cases, due to the development of new plaques inside the stent (restenosis). If a carotid-subclavian bypass operation was performed, then the probability of relapse is no more than 2% of cases.
Angioplasty and stenting of the subclavian arteries
Subclavian arteries
Subclavian arteries
- These are large vessels that carry blood to both upper extremities.
Rice. Subclavian artery
Atherosclerotic lesions of the subclavian arteries are quite common and can lead to strokes or thrombosis of the arteries of the upper extremities, followed by possible amputation.
Also, with this pathology, the so-called “steal” syndrome, or “steal” syndrome, when blood flows through the vertebral artery into the subclavian artery, after which cerebral ischemia may develop.
About the angioplasty and stenting procedure
Today, the most effective methods of treating severe narrowing of the subclavian arteries are balloon angioplasty and stenting. These are the most gentle and organ-preserving treatment methods that do not require open surgery and anesthesia. The procedure is painless and takes place under local anesthesia. Surgeries allow you to restore the lumen of narrowed arteries using special balloon catheters and stents.
In recent years, isolated angioplasty of the subclavian arteries has been used very rarely, because Stent implantation is almost always more effective.
What is a stent?
Stent
- a cylindrical endoprosthesis, laser cut from a solid metal tube. Subsequently, it is attached to a special balloon catheter, and in a compressed state it moves along the course of the altered subclavian artery.
When the stent is installed in the area of narrowing of the artery, control angiography
to confirm optimal positioning of the stent, and then deploy it under high pressure. In case of incomplete deployment of the stent, angioplasty of the stented area will be performed with a special catheter with a balloon at the end to achieve an optimal result.
Rice. Angiography with stenting of the subclavian artery
Indications and contraindications
Indications
for angioplasty and stenting of the subclavian arteries: symptomatic stenoses (narrowing) more than 50% and asymptomatic stenoses more than 75%. Symptoms of narrowing of the subclavian arteries are weakness in the affected arm, sometimes necrosis of the fingers or gangrene of the hand.
Contraindications:
- total occlusion of the vessel (in relation to the internal carotid artery);
- vascular diseases preventing the use of endovascular instruments
Preoperative examination and preparation
Before you begin treatment for subclavian artery stenosis, you must first diagnose it and confirm the diagnosis. To do this, we use the following research methods:
- Ultrasound diagnostics
- Computed tomography with vessel contrast;
- X-ray of the lungs.
Additionally, general clinical blood and urine tests and biochemical blood tests are performed. It is necessary to perform endoscopy of the stomach to exclude ulcers, since after surgery antithrombotic drugs are prescribed, which can provoke gastric bleeding in case of ulcers.
Where are stenting operations performed in Kyrgyzstan?
Angioplasty and subclavian artery stenting operations are performed in the following clinics:
- MC "Cardio-Asia Plus";
- Research Institute of Heart Surgery and Organ Transplantation;
- Southern Regional Scientific Center for Cardiovascular Surgery (
URRCSS )
These clinics have accumulated a lot of experience in stenting complex lesions of the subclavian arteries, including recanalization of extended occlusions (when the subclavian artery is closed over a long distance).
Prognosis after angioplasty and stenting of the subclavian arteries
After successful angioplasty and stenting of the subclavian artery, the likelihood of re-stenosis is significantly reduced, rapid recovery of the body occurs, and good long-term results are predicted. A huge advantage of these interventions is that there is no need to open the sternum or make an incision in the neck, as when performing bypass and other open operations, but only a small puncture (about 2 mm) at the site of catheter insertion.
Observations after angioplasty and stenting of the subclavian arteries
After this surgical intervention it is recommended:
- Give up bad habits, especially smoking.
- If necessary, control your eating behavior: exclude fatty, smoked, salty foods.
- Lose weight if you are overweight.
- Perform dosed physical activity daily.
- If possible, spend more time in the fresh air.
- Avoid stress!
- Take medications recommended by your doctor.
- Visit your doctor at recommended intervals!
- If you experience any discomfort in your body, consult a doctor.
Is stenting of the subclavian arteries performed in Kyrgyzstan?
In our country, such operations are carried out in several medical institutions. Among them:
- MC "Cardio-Asia Plus"
- NIIHSTO (Research Institute of Heart Surgery and Organ Transplantation).
At NIIHSTO, stenting operations are performed by an experienced cardiac surgeon-arrhythmologist, head of the department of X-ray endovascular surgery, Turdubaev Abay Kubanychbekovich.
Rice. Cardiac surgeon-arrhythmologist Abay Turdubaev
At the Cardio-Asia Plus MC, highly qualified endovascular surgeon Eraliev Talant Kakanovich performs operations.
!! Many operations are performed in our country and now there is no need to travel abroad.
Rice. Endovascular surgeon Talant Eraliev
These medical institutions have everything necessary to perform angiography and stenting. Patients at high risk who seek help prevent the development of stroke, preserve their life and improve its quality.